
Much to our pleasant surprise here at CCF, the recent health care debate elevated and educated many lawmakers on the role of Medicaid for children and families. Medicaid, of course, is the foundation of health coverage for children in the U.S.—a fact that was often overlooked until recently, even by health-savvy lawmakers. But Say Ahhh! readers know that our nation’s historic success in covering kids also depends upon Medicaid’s small but mighty partner, the Children’s Health Insurance Program (CHIP), which has served as a catalyst for kids’ coverage gains alongside Medicaid since it was created in 1997.
Right now, children, families and states face grave uncertainty about CHIP’s future, since no new federal funds will be available after September without Congressional action.
Because we’ve all been mired in the Medicaid debate, it’s a good time to remind lawmakers about CHIP and its importance to kids. In turn, we are refreshing our CHIP resources and education materials. CHIP was created I997 to help states provide affordable coverage to uninsured children in middle-income families who didn’t qualify for Medicaid but for whom private coverage was out of reach. Our updated “ About CHIP page “(also as PDF primer) provides more of the basics. Here are the top things lawmakers and child health stakeholders need to know.
CHIP is a federally funded, state-administered block grant that serves nearly 9 million children during the course of a year. CHIP allows states to offer coverage to children at higher income levels that do not qualify for Medicaid. As a result, the median income eligibility for children’s coverage in states is 255% of the federal poverty line (FPL), with states ranging from 175% FPL (Wyoming) to 405% FPL (New York). States administer CHIP with even more flexibility than in Medicaid to set income eligibility, design benefits, set cost-sharing levels, and establish enrollment procedures within broad federal parameters. Many states, notably, have designed their CHIP programs within Medicaid or nearly identical to Medicaid, particularly in terms of covered benefits. Which leads me to one of our favorite points…
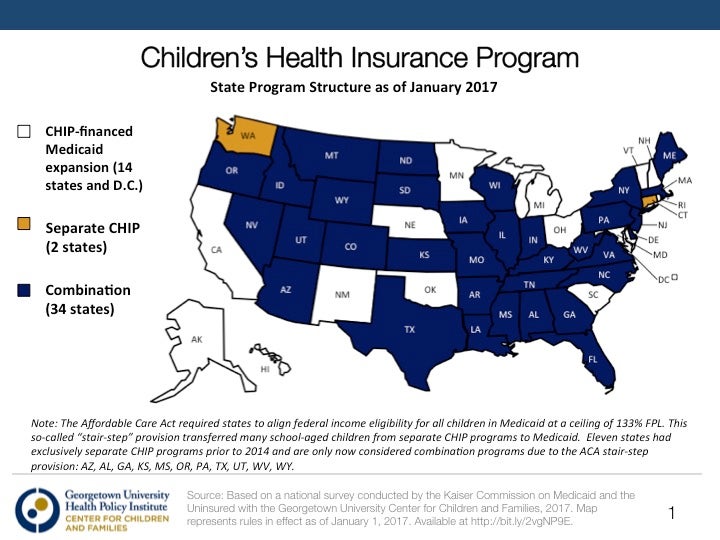
CHIP works together with Medicaid to provide coverage by serving more middle income children—in many states Medicaid and CHIP are indistinguishable. CHIP and Medicaid are like peanut butter and jelly, or peas and carrots, two sides of the same coin—you take your analogy! The point is they work together. Medicaid plays the outsized children’s coverage role, with more than 37 million in the program, versus 9 million served by CHIP (See chart below). CHIP gives states the option to create a separate CHIP program that sits on top of Medicaid, extend Medicaid to children and higher income levels with funding through CHIP, or some combination of the two. In 2017, 14 states run pure CHIP-funded Medicaid extensions, 2 states run exclusively separate programs, and 34 states administer some combination of the two. What does this mean? More than half of CHIP-funded children are in Medicaid—they receive full Medicaid EPSDT benefits and are not in a separate program.

Unlike Medicaid, Congress has to come back to extend CHIP funding every few years. The longer the funding extension, the better it is for financial planning and budgeting by state policymakers and families. In 1997, CHIP was authorized for 10 years. In 2009, Congress passed the CHIP Reauthorization Act (CHIPRA), which added another 4.5 years of funding, more pathways to additional funds for states reaching their limit, and new tools and incentives to reach more children and measure Medicaid and CHIP quality.
In recent years, CHIP has been subjected to a number of short-term extensions that create more financial uncertainty for families and state leaders trying to balance their budgets and meet the health care needs of residents of their states. The Affordable Care Act (ACA) extended CHIP funding for an additional two years to 2015, and the 2015 Medicare and CHIP Reauthorization Act (MACRA) extended funding through September 30, 2017 (Yes—that’s less than two months away!). The uncertainty that state CHIP directors and budget staff are facing right now is a good example of why CHIP should be extended for longer periods of time and well ahead of the funding expiration deadline. States need enough lead time to plan for the possible end of federal funds or their renewal—crafting notices to families, renewing or phasing out managed care plan contracts, seeking to connect children to other coverage sources if separate CHIP programs end…. Many states have public notice requirements for CHIP with time frames that range from 30 days to 100 days prior to implementing a change in the program. Many families, as a result, are sitting squarely in the face of this uncertainty with their children’s coverage on the line.
States receive a higher federal match for CHIP-covered/-funded children. Like Medicaid, the federal government pays a share of the cost of services for CHIP children (unlike Medicaid, of course, the federal funds are capped). Since 1997, the federal CHIP match rate has been 30 percent higher than Medicaid, ranging from 65 to 82 percent. The ACA authorized and MACRA funded an additional 23-percentage point CHIP match boost up to a maximum of 100% in effect today. Extending this bump through 2019 as the ACA intended is another key question to consider during debate over CHIP’s extension. The National Academy for State Health Policy reports that most states are counting on this additional match through 2019.
The clock is ticking… All eyes are on Congress for next steps as September 30th approaches and lawmakers ready themselves for recess. A 5+ year, clean extension would give peace of mind to many families and states alike.
Editor’s note: Read more about the future of CHIP as the program turns 20



{kind=link}