
If we consider what children need as part of their healthy development, prevention and early intervention are most important. Children’s experiences, especially in the earliest years of rapid brain development, have an incredible impact on long-term health outcomes. And those same experiences are impacted by their parents’ health.
The latest illustration: The opioid epidemic, which is tearing families and communities apart in many states. New analysis from our friends at the United Hospital Fund and Boston Consulting Group unpacked the number of children affected by opioid use disorder (OUD), and the resulting costs over a decade-plus period.
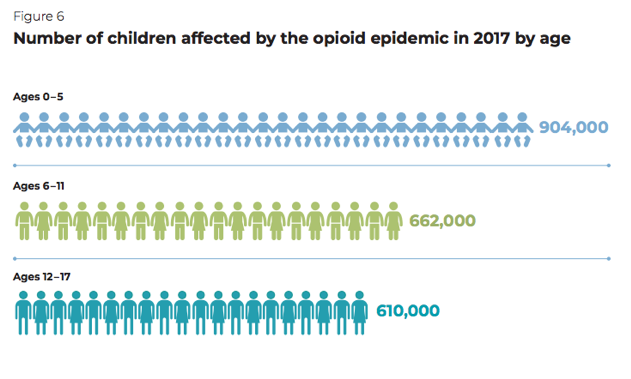
The Ripple Effect: National and State Estimates of the U.S. Opioid Epidemic’s Impact on Children explores the demographics for the estimated 2.2 million children in 2017 whose parents suffer from OUD or experienced OUD themselves. Young children are especially hard hit: Most are under the age of 12, and nearly a million are preschool-aged (see figure below). No state is immune: West Virginia and New Hampshire experience the highest per capita rates of children affected, four populous states (California, Florida, New York, Texas) have low rates but nearly 30 percent of the total number of children impacted.
More troubling, the authors estimate that even if the recent downward trends in OUD continue, the number of children impacted will still increase to more than 4 million by 2030.
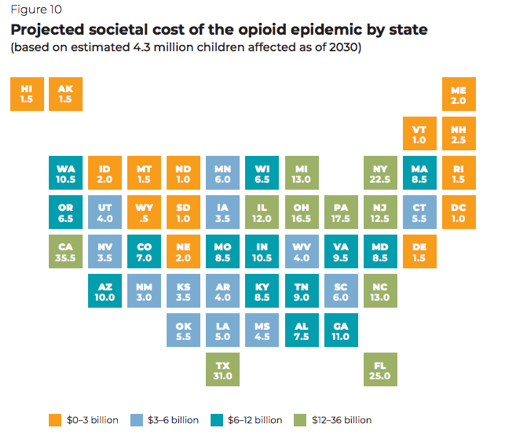
Many Say Ahhh! readers know that substance use exposure is one adverse childhood experience (ACE) that can make children susceptible to additional adversity. The more ACEs a child experiences, the more vulnerable they are to poor health, social, and economic outcomes well into adulthood. The chartbook estimates that OUD’s impact alone—and notably NOT the full range of possible substance use disorders that could impact families – will cost the U.S. as much as $400 billion in 2030 in added costs for these children in the health care, special education, child welfare, and criminal justice systems.
Curious about your state? The figure below estimates 2030 costs. The sourcebook also includes a detailed appendix with additional state-level data that is sure to interest many child health leaders.
So what now? The report makes a number of recommendations that federal and state policymakers are taking steps to address. Following are those where Medicaid can and should lead as a player and payer of prevention and early response services for children and their families (p. 14):
- Coordinate the response across health care, law enforcement, child welfare agencies, and schools, so families struggling with substance use disorder receive a “no-wrong-door” approach to evidence-based services. Is Medicaid an engaged player at the table alongside other systems? How is Medicaid case management employed for care coordination? Is the referral system and feedback loop well-understood and employed across systems?
- Provide kinship caregivers and foster parents with tools for responding to trauma in children. More than a dozen states, for example, allow Medicaid to pay for parenting programs with the express goal of improving a child’s social and emotional development.
- Increase the availability of family-based mental health services. In 42 states Medicaid pays for dyadic, or parent-child, treatment. States like New York are seeking ways to allow a parent risk factor or diagnosis, such as OUD, qualify for dyadic treatment and other two-generation approaches under a child’s Medicaid enrollment.
- Encourage integrated health and social services that simultaneously meet the needs of parents and children. Does Medicaid help to support this approach in alignment with social services agencies? Are Medicaid managed care organizations required or incentivized to help create needed linkages?
- Reduce geographic and racial/ethnic disparities in access to services.
Underpinning all of these recommendations is the important role Medicaid expansion can play. Right now, 14 states can move uninsured parents and other adults one step closer to any substance abuse or mental health prevention or treatment services they may need by expanding Medicaid. Once more for those in the back: Children don’t live in isolation — the health of their parents and caregivers in inextricably linked to their development. Failure to act on this knowledge puts children at incredible risk for a host of avoidable challenges throughout their lives. Medicaid expansion is an investment in children, not just uninsured adults.
For children themselves, we know we can do much more in Medicaid, where prevention and early intervention is baked into pediatric benefits under EPSDT. As health system leaders look toward paying more for value, it is imperative that we consider costs over the long-term and well beyond the health care system. If we care about long-term outcomes (and savings beyond next year!), this report adds more credibility to the argument that the health system—and other systems, not to mention opioid settlement dollars!— should invest more upfront for kids. Much has been done, much more is needed.