Executive Summary
Enrollment in Medicaid has grown significantly during the coronavirus pandemic. Provisions in the Families First Coronavirus Response Act (FFCRA) require states to provide continuous coverage for Medicaid enrollees until the end of the month in which the public health emergency (PHE) ends in order to receive enhanced federal funding. Continuous enrollment has helped to preserve coverage and halted Medicaid churn. However, when the PHE ends, states will begin processing redeterminations and millions of people could lose coverage if they are no longer eligible or face administrative barriers despite remaining eligible. Existing state enrollment and renewal procedures, as well as their approaches to the unwinding of the continuous enrollment requirement, will have major implications for Medicaid enrollment and broader coverage.
The 20th annual survey of state Medicaid and Children’s Health Insurance Program (CHIP) officials conducted by KFF and the Georgetown University Center for Children and Families in January 2022 presents a snapshot of actions states are taking to prepare for the lifting of the continuous enrollment requirement, as well as key state Medicaid enrollment and renewal procedures in place during the PHE. The Centers for Medicare and Medicaid Services (CMS) released new guidance on March 3, 2022, which emphasizes promoting continuity of coverage and avoiding inappropriate coverage terminations when the continuous enrollment requirement ends. While this recent guidance was released after the survey was fielded, state responses reported here illustrate how states expect to approach the unwinding of continuous enrollment and what the effects of the new guidance may be.
Plans for the End of the PHE
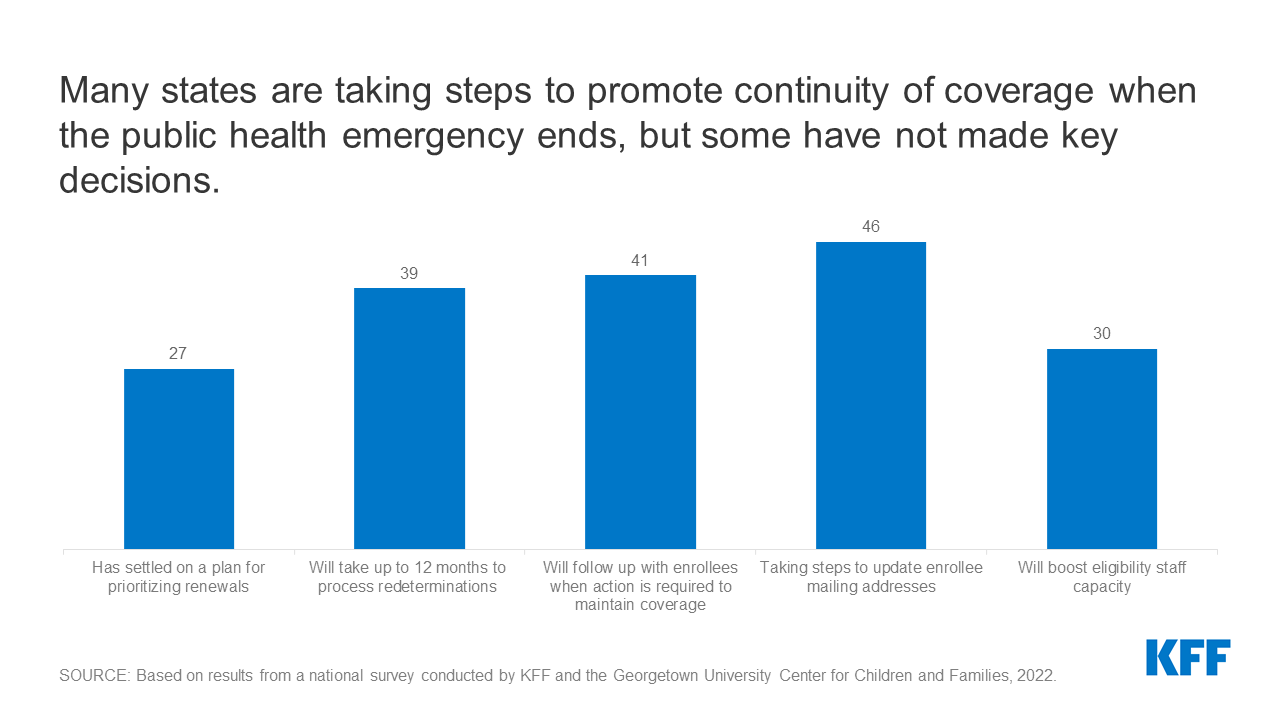
States are required to develop plans for how they will prioritize outstanding eligibility and renewal actions when the continuous coverage requirement is lifted; just over half of states (27) have determined their approach. At the time of the survey, given uncertainty around the timing of the end of the PHE, timing of additional guidance from the CMS, and the future of the Build Back Better Act, it is perhaps not surprising that many states have yet to finalize their plans. However, having plans in place early will allow for better preparation and will enable states to communicate their plans to enrollees and other stakeholders in the state. Among the states with plans, eleven states indicate they will target individuals who appear to be no longer eligible first, while nine states plan to conduct fresh renewals based on the individual’s renewal month, and seven have adopted a combination or hybrid approach. While most states plan to wait until the continuous enrollment requirement is lifted to resume disenrollments, three states have not yet decided whether they will forgo enhanced federal funding and begin disenrollments before the end of the PHE. However, even if states begin disenrollments prior to the end of the PHE, they must still follow the unwinding guidance CMS has issued.
Fifteen states indicate they will conduct electronic data matches to identify and target enrollees for priority action who may no longer be eligible after the continuous enrollment requirement is lifted. States are not required to conduct data matches in between renewal periods. While data matches can identify people who experienced a change in income or circumstance that makes them no longer eligible, broad data searches may also identify inconsistent or inaccurate information that does not impact eligibility and could lead to eligible individuals losing coverage if they do not follow up.
The majority of states (39) plan to take up to a full year to process redeterminations and return to routine operations; however, nine states plan to resume normal operations more quickly. When states resume redeterminations at the end of the PHE, they will need to conduct a fresh review of eligibility based on current circumstances before disenrolling anyone from Medicaid. Current CMS guidance gives states up to 12 months to initiate and 14 months to complete all redeterminations and 39 states indicate they will take at least 9 months and up to the full year. The elimination of the enhanced federal Medicaid matching rate (at the end of the quarter in which the PHE ends) could put fiscal or political pressure on states to move more quickly. The risk of moving quickly is that there will be less time to conduct outreach to enrollees and develop staff capacity to process renewals. CMS encourages states to initiate redetermination on no more than 1/9th of their total caseload each month to minimize this risk.
When the continuous enrollment requirement is lifted, a majority of states (41) plan to follow-up with enrollees when action must be taken to avoid a loss of coverage due to missing information. States are not required to follow up with enrollees who do not respond to a renewal request and may simply send a termination notice if no response is received within 30 days. However, sending reminder notices via mail – and also through other communication modes, such as phone, text, and/or email – can increase the response rate to renewal requests and reduce the number of people who remain eligible but are disenrolled at the end of the PHE because they did not respond to a request for information.
In preparation for the end of the PHE, states are taking steps to update enrollee mailing addresses. The two-year COVID-19 emergency has likely exacerbated longstanding difficulties in reaching enrollees by mail. In response, the vast majority of states (46) are planning actions to update mailing addresses before the end of the PHE, including conducting data matches with the United States Postal Service (USPS) National Change of Address database; working with managed care organizations (MCOs); and conducting outreach campaigns. In addition, 35 states will follow-up on returned mail to attempt to locate an enrollee before terminating coverage.
Anticipating the need for additional staff resources at the end of the PHE, 30 states plan to take steps to boost staff capacity. Most states are taking multiple actions that include approving overtime, hiring new eligibility workers or contractors, or borrowing staff from other units or agencies.
Most states are able to report key metrics needed to monitor the unwinding process. Almost all states (50) report they are capable of tracking call center statistics and a majority (41) are able to report the share of disenrollments that were determined ineligible versus disenrollments due to procedural reasons. Having timely and reliable data from states will be needed to monitor the unwinding process and assess whether additional steps should be taken to avoid coverage losses among those who remain eligible. In recent guidance, CMS has indicated it will require states to report monthly data to monitor their progress on unwinding and compliance with current rules, although there is no indication the data will be released publicly.
In 20 states able to report, it is estimated that about 13% of Medicaid enrollees will be disenrolled when the continuous enrollment requirement ends. However, the estimates range widely across reporting states from about 8% to over 30% of total enrollees. Based on available data, most states report that an increase in income will be the primary reason for the disenrollment although several states also expect incomplete renewals or missing documentation will be a primary reason for disenrollment. If these estimates hold true, millions of people will lose Medicaid coverage in the months following the end of the PHE; however, many children will likely be eligible for CHIP and many adults will likely be eligible for Affordable Care Act (ACA) Marketplace or other coverage. Successfully transitioning these individuals into those other coverage options could avoid gaps in coverage and reduce the number who lose coverage altogether and become uninsured.
Enrollment and Renewal Policies During the PHE
Even during the PHE, states continue to streamline application processes and integrate non-MAGI and non-health programs into the system that determines MAGI Medicaid eligibility. In almost all states, applications can be submitted online, by telephone, in person, or by mail. Additionally, nearly all states (48) now offer online accounts for Medicaid and CHIP enrollees that make it easier for individuals to submit and access information about their coverage. States have taken steps to improve the mobile friendliness of their applications and online accounts. All states use electronic data matches from a variety of data sources to verify income eligibility and, as a result, most states (43) can provide eligibility determinations in real time (within 24 hours).
While states cannot disenroll people, as of January 2022, most states (42) report processing ex parte renewals and sending renewal forms (30 states) to reduce backlogs in renewals at the end of the PHE. By continuing ex parte renewals during the PHE, states have been able to renew coverage for 12 months for those who remain eligible. Of the 42 states actively processing ex parte renewals, nearly two-thirds (30 states) are sending renewal forms or requests for documentation when they are unable to confirm ongoing eligibility through electronic data sources, although they may not disenroll anyone during the PHE. By processing ex parte renewals and sending out renewal forms, states will have a smaller backlog of delayed renewals or pending actions when the PHE ends.
Medicaid and CHIP Eligibility
As of January 2022, Medicaid and CHIP eligibility was stable as the PHE protections remained in effect for the entirety of 2021. Oklahoma and Missouri implemented the ACA Medicaid adult expansion in 2021, leaving only 12 states that have not filled the coverage gap for low-income adults. In the 12 states that have not implemented the Medicaid expansion, eligibility for parents remains extremely low (ranging from 16% to 100% of the poverty level) and only Wisconsin covers adults without dependent children (through a waiver of standard Medicaid eligibility rules). Eligibility levels for children and pregnant women held constant with median eligibility at 255% of the federal poverty level (FPL) and 205% FPL respectively.
Looking Ahead
Recent CMS guidance provides guardrails and flexibilities for states to promote continuity of coverage during the unwinding period; however, state decisions and actions will have implications for Medicaid enrollment. Recently released guidance emphasizes strategies to promote continuity of coverage. The guidance reiterates existing options for states, such as adopting 12-month continuous eligibility for children and extending postpartum coverage for 12 months, and provides additional flexibilities, including using Supplemental Nutrition Assistance Program (SNAP) eligibility to renew Medicaid coverage. How states approach the unwinding of the continuous enrollment requirement will affect the extent to which eligible individuals retain coverage and those who are no longer eligible are able to transition to other coverage. Outcomes will differ across states as they make different choices and careful monitoring of state progress throughout the unwinding period can provide information to assess fiscal effects and state efforts to promote continuity of coverage.
The fate of the Build Back Better Act (BBBA) will have implications for overall coverage. The BBBA includes provisions to close the Medicaid coverage gap in states that have not adopted the ACA Medicaid expansion and to extend the enhanced Marketplace premium subsidies initially made available by the American Rescue Plan Act (ARPA), which have made coverage more affordable for millions of people. While the number of people who are uninsured has not increased during the PHE as many had predicted, millions of people could lose coverage if those who continue to be eligible for Medicaid are not able to retain coverage, and if the provisions in the BBBA that close the coverage gap and make Marketplace coverage more affordable are not enacted.