The Kaiser Family Foundation (KFF) and Georgetown University Center for Children and Families annual 50-State Survey on Medicaid and CHIP Eligibility and Enrollment was released today. The survey focuses on state policies impacting children, pregnant individuals, parents, and other non-elderly adults whose Medicaid eligibility is based on financial eligibility rules. This year’s survey provides a snapshot of state actions at a watershed moment for Medicaid.
The annual survey, now in its 21st year, doesn’t often qualify as “breaking news” but as policymakers, members of the media, advocates, and stakeholders try to get their arms around the lifting of the Medicaid continuous enrollment requirement that begins on April 1, this year’s survey may just fall into that category. The pandemic-era Medicaid continuous coverage protection expires on March 31 and states are allowed to start disenrollments after conducting a full review of eligibility. As states begin to wind down the continuous enrollment provision, a number of people will likely no longer be eligible for Medicaid while others will likely face administrative barriers and lose coverage despite being eligible. States face the challenge of how to disenroll those who are no longer eligible while keeping eligible people enrolled, as we have explained in greater detail in numerous blogs and reports.
This year’s survey shows the efforts states have taken to prepare for the unwinding as well as broader policy changes to improve existing eligibility, enrollment, and renewal procedures. Here are the highlights of the key findings:
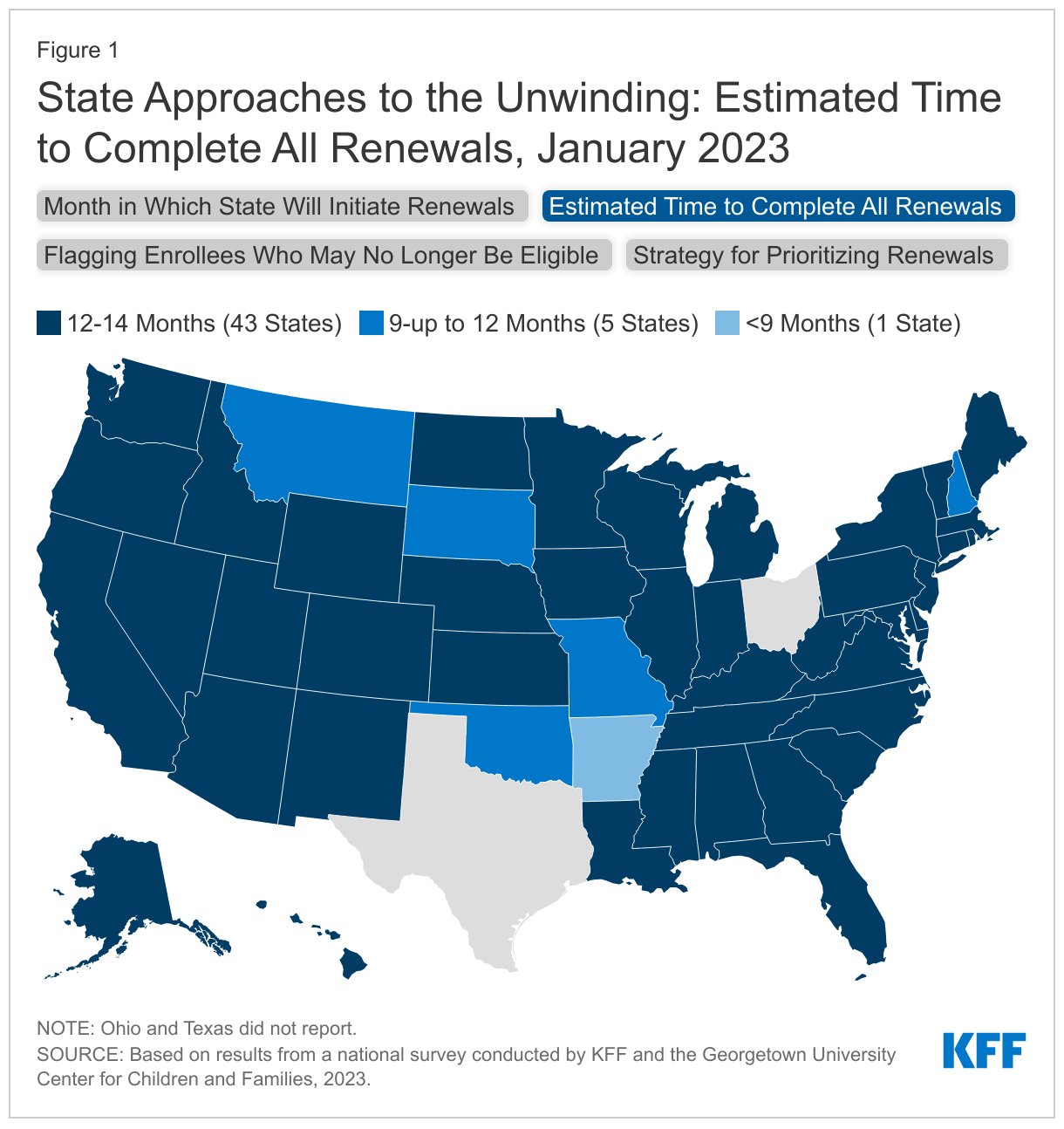
- States are adopting a range of approaches to unwinding the continuous enrollment provision, though most are taking as much time as possible to complete the process. Most states are waiting until March or April to initiate their “unwinding” plans while 43 of the 49 reporting states plan to spread renewals over 12 to 14 months. Taking more time to initiate and complete the unwinding process can help to avoid overwhelming staff resources and prevent inappropriate terminations. Additionally, more than two-thirds of the states (35 of 49 reporting states) are adopting an approach to prioritizing renewals that considers multiple factors, including time since last renewal and potential ineligibility.
- A majority of states (43) have continued to process ex parte renewals over the past year and over half (30 states) have taken steps to increase the share of renewals completed via ex parte. Ex parte renewals reduce administrative burden on both states and enrollees and can lower the number of disenrollments that occur because an enrollee is unable to complete the renewal process. Of the 38 states reporting ex parte rates, 18 states are successfully processing more than half of renewals using ex parte processes, up from 11 states in 2022.
- The unprecedented volume of work ahead comes at a time when most states face significant staffing challenges. More than half of reporting states have staff vacancy rates greater than 10% for frontline eligibility workers (16 of 26 reporting states) and slightly less than half for call center staff (13 of 28 reporting states). States are adopting multiple strategies to address eligibility staffing shortages, including approving overtime and hiring new staff, temporary workers, or contractors.
- Most states are taking an all-encompassing approach to ensuring enrollees can be reached with important renewal information and other notices during the unwinding. All states have taken action to encourage enrollees to update their contact information, with the majority taking a multi-pronged approach. A majority of states (41) are engaging managed care organizations (MCOs) to conduct outreach and assist members. Once renewals are sent out, over two thirds of states (36) plan to follow-up with enrollees when action is required to maintain coverage.
- During the pandemic, states have taken actions to improve maternal and immigrant coverage while several states are moving toward providing multi-year continuous eligibility for children. More than two-thirds of states (37) have now extended or plan to extend postpartum coverage for a full 12-months post pregnancy. Kentucky and Oklahoma increased income eligibility levels for pregnancy coverage. Kentucky also removed the five-year bar for pregnancy coverage of lawfully-residing immigrants in Medicaid and CHIP. Connecticut and Maine adopted the CHIP “unborn child option”, effectively providing pregnancy coverage regardless of immigration status. Connecticut, Maine, New Jersey, Rhode Island, and Vermont are now using state funds to cover children regardless of immigration status. Additionally, several states are working to provide continuous eligibility to children for longer periods. Oregon became the first state to receive approval to cover children continuously until their sixth birthday; three other states, California, New Mexico, and Washington, have similar plans. Oregon also received approval to provide two-year continuous coverage for all other enrollees, a policy that Illinois is planning to adopt for all age groups.
Many factors will impact how well a state navigates the unwinding process including system capabilities, ex parte renewal rates, communications strategies, staff capacity; and adoption of operational policies that make it easier for eligible people to stay enrolled. Other important factors influencing coverage include whether or not a state has taken steps to address gaps in coverage by putting in place continuous coverage policies, taken action to improve maternal and immigrant coverage and adopted Medicaid expansion. We look forward to highlighting these and other state health coverage policies in future blogs.