
Those of us in child health policy are familiar with the argument that coverage is important to children to ensure preventive care that can catch and address disease and delays early before they become larger hurdles. But once kids are covered, unpacking how and whether that preventive care is achieved, and defining the steps, policy levers, and players in this process is not simple. Exhibit A: Developmental screening. Our new brief outlines key issues surrounding developmental screening in Medicaid and CHIP. It is a critical first step to see if young children are meeting key developmental milestones, recommended by AAP’s Bright Futures to be performed at the 9-, 18- and 30-month well-child visits. Results of a screen determine whether a child will go on to receive a more detailed evaluation, which could lead to additional services, such as early intervention (IDEA Part C) or other related therapy services.
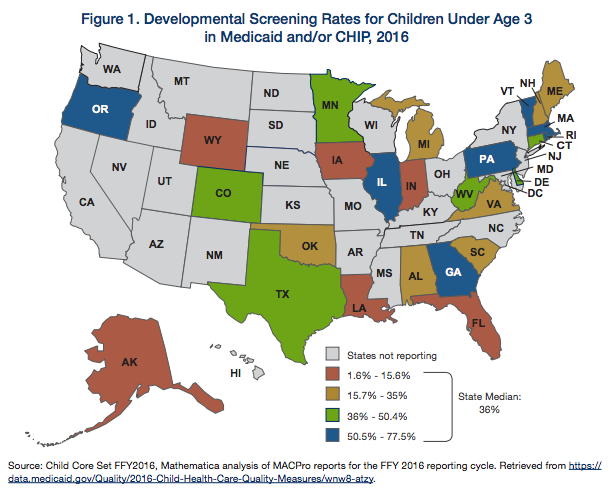
As our quality guru Tricia Brooks blogged last fall, more than half of states reported, for the first time in 2016, on their developmental screening measure in Medicaid and/or CHIP as part of the Child Core Set. This means we finally got to see the reported percentage of children under age three receiving developmental screens. The result? Of the 26 states reporting in 2016, developmental screening rates for children under age 3 in Medicaid and/or CHIP ranged from 1.6 percent in Alaska to 77.5 percent in Massachusetts, with a median of 36 percent.
Important disclaimer here: A “developmental screening” is more than just the regular observation that a physician or other professional uses to determine whether a child is physically or social-emotionally on track. In practice and according to the AAP standard, it’s much more specific: use of a validated, standardized tool during well-child visits at regular intervals to determine if a child is meeting developmental milestones at various ages and stages. This distinction is important, since it’s not uncommon to hear stakeholders refer to “EPSDT screen” and “developmental screen” interchangeably. In this case, developmental screening is much more specific, and distinct from other important health screenings, such as vision or hearing screening.
What can we learn from this? Well, the wide variation in state rates of developmental screening suggests lots of room for improvement in rates themselves. A very low rate may reflect a need to educate providers on the importance of using a validated, standardized screening tool that counts as a developmental screen for the purpose of measure reporting. In addition, since the measure relies on Medicaid billing and claims data, the variation in rates may also reflect differences in billing practices, where perhaps more screens are actually occurring but not reflected in billing data.
The good news for early childhood and health policy stakeholders?
- We have baseline state data in Medicaid and CHIP for developmental screening. It may not be perfect, but it exists!
- There is an opportunity to encourage more states to report the developmental screening measure for Medicaid and CHIP. Not to mention, since states will be required to report all measures in the Child Core Set starting in 2024 –– why not start now to establish a baseline and familiarity with collecting and improving necessary data?
There’s a lot to unpack here and much more still to learn on this topic. We hope to use future briefs and blogs to consider how advocates can advance developmental screening in Medicaid and CHIP, better understand the Child Core Set measure and its utility, and identify opportunities for advocates and policymakers to use data and policy to look well beyond screenings to ensure follow-up referrals and needed services are happening as a result. Just like a screening, this brief is just the first step.
Michael Odeh is the Director of Health Policy for Children Now in California. He is a former Georgetown University CCF staff member.