Passage of the budget reconciliation law signed into law by President Trump (HR1) will result in a gross reduction of $990 billion in federal Medicaid and CHIP spending over 10 years and an increase in the number of uninsured Americans of 10 million. These are the largest health cuts in Medicaid’s history, and passage of the bill was delayed by worries that rural hospitals across the United States would be put at further risk of closing because so many of their patients rely on Medicaid. KFF estimates that HR1 will reduce federal Medicaid spending in rural areas across all states by $137 billion over 10 years.
To ensure passage, Congress included a $50 billion “Rural Health Transformation Fund” (or RHTF). For more information see our other CCF blogs on the RHTF including background, analysis of the state application process, the need to address maternal health shortages, and the importance of addressing the needs of children and families in rural areas. While there was nothing in the bill’s language in HR1 requiring that the funding in the RHTF be provided to rural hospitals to protect them from large Medicaid cuts, there was also no prohibition against states using RHTF funding for that purpose—and members of Congress who voted yes in the end repeatedly cited the fund’s ability to protect their rural hospitals.
Unfortunately, the ambiguity members of Congress left in HR1 about whether or not to actually help fund rural hospitals and health clinics was resolved last month by the federal Centers for Medicare and Medicaid Service (CMS). CMS released the state “Notice of Funding Opportunity” detailing for states how they could apply for RHTF funds and what the restrictions would be. CMS lists as a condition of funding that states cannot exceed use of 15% of federal funding awarded to the state for health provider payments – including payments to rural hospitals.
This limitation on funding should come as a surprise to many of the politicians who took every opportunity to characterize their support for a bill with the largest health care cuts in Medicaid’s history as actually support for rural hospitals in their states.
For example, Senate Finance Committee Chair Mike Crapo (R-Idaho) characterized the funding as the “$50 billion rural hospital fund” [Emphasis added] and said it was “arguably the single largest investment in rural health care in more than 20 years.” Likewise Senator John Barrasso (R-WY) used similar language about the fund, calling it the “rural hospital fund” with “$50 billion designated for rural hospitals all across America.” And Senator Jerry Moran (R-Kansas) characterized HR1 as creating “a $50 billion fund to provide emergency assistance for rural hospitals at risk of closure…” while Representative Jule Fedorchak (R-North Dakota) also characterized the program as the “Rural Hospital Fund.” Senator Lisa Murkowski (R-Alaska) only voted for the bill after the RHTF was increased to an amount she felt could help prevent rural Alaska hospitals from closing. And Senator Josh Hawley (R-Missouri) reversed his opposition to the bill after what was characterized as the “$50 billion rural hospital fund” was included.
This assumption that the RHTF was primarily about helping rural hospitals was taken up by state legislative officials as well. For example, in Ohio, “Ohio House Speaker Matt Huffman, R-Lima, told The Dispatch that he thinks rural, independent hospitals should get the most of the money coming Ohio’s way.” [Emphasis added.]
In the end, what was characterized by many as a “rural hospital fund” is really nothing of the sort. The vast majority of RHTF funding is actually prohibited from directly benefiting health care providers, including rural hospitals. Members of Congress may have had different motivations for passing HR1, but the implementation of the law around the RHTF is different than the assurances around help for rural hospitals many policymakers gave the public.
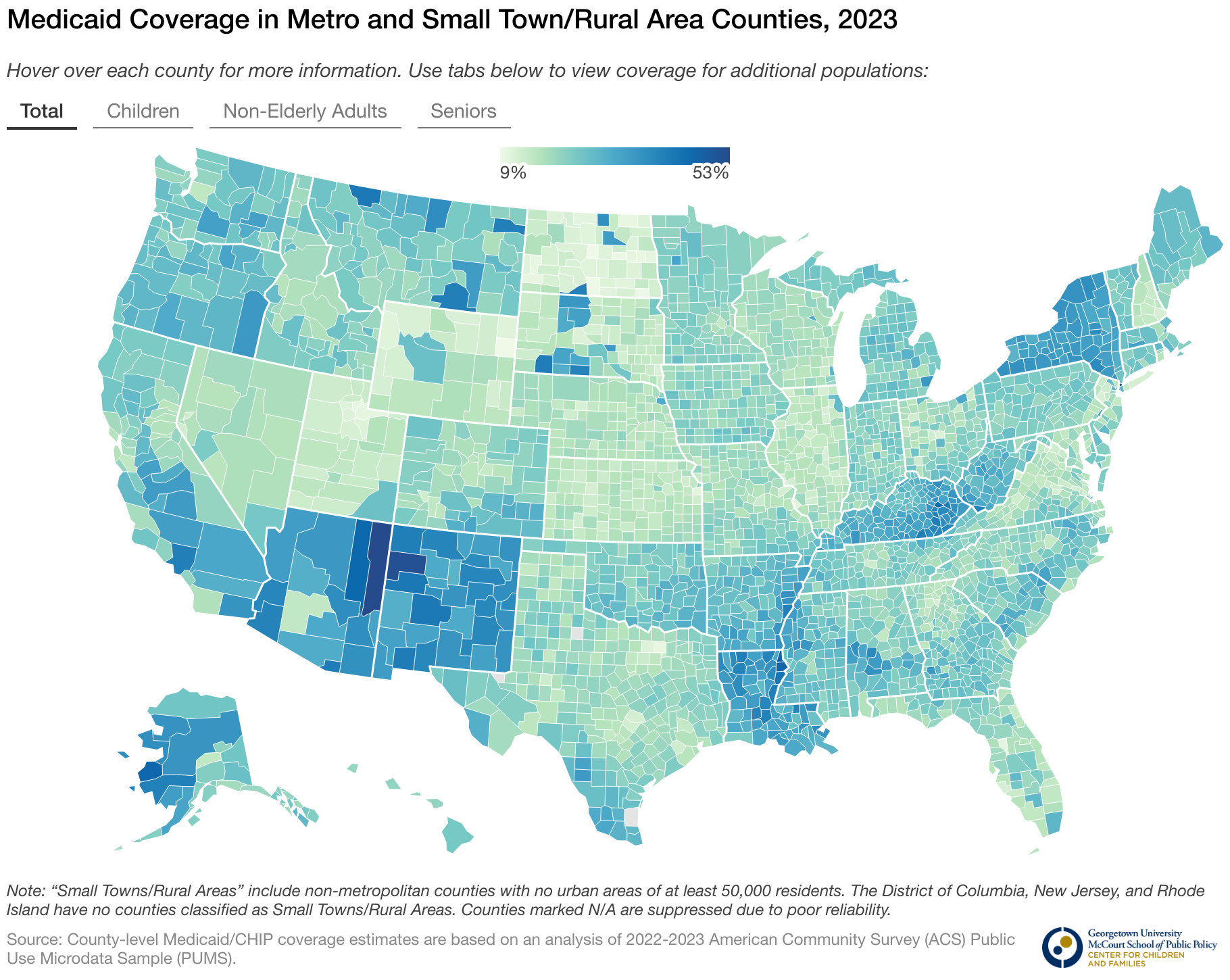
[Editor’s Note: The Georgetown University Center for Children and Families Rural Health Policy Project report published earlier this year found that non-elderly adults and children living in rural areas and small towns are more likely than those living in metro areas to rely on Medicaid for their health insurance. As a consequence, cuts to federal Medicaid funding and other changes to Medicaid being contemplated in Congress will cause harm everywhere, but are more likely to cause greater harm to rural communities and small towns than metro areas. View interactive state maps showing Medicaid coverage in rural areas here.]