On June 1, 2026, the Centers for Medicare & Medicaid Services (CMS), published the Interim Final Rule with Comment (CMS-2454-IFC, hereafter referred to as the IFR) “Medicaid Program; Community Engagement Requirement for Certain Individuals” as required by the 2025 Budget Reconciliation Law (hereafter referred to as H.R. 1). States that have expanded Medicaid to adults – whether through the Affordable Care Act (ACA, Section 1902(a)(10(A)(i)(VIII) of the Social Security Act) or a Section 1115(a)(2) waiver – must implement this consequential shift in policy, commonly referred to as work reporting requirements (WRR). Prior state experience has shown that requiring individuals to report work or qualifying activities results in significant coverage losses resulting from the confusion and the administrative burden for eligible and enrolled individuals. Notably, the IFR establishes a complex set of definitions and processes that are much harsher and more difficult to implement than was stipulated in H.R. 1.
H.R. 1 puts unreasonable deadline pressure on states by setting an extremely tight timeline for implementing such a significant policy at the same time states also must implement semi-annual renewals for expansion adults among other major policy changes. The IFR further complicated state implementation by narrowing certain definitions and adding requirements not specified in H.R. 1, particularly relating to medical frailty and the use of self-attestation. The IFR caught states off guard by deviating from informal guidance and technical assistance that CMS had been giving states for months and setting back progress states had made in planning, implementing system changes, and managing costs. In other areas, CMS declined to define certain terms while warning states about forthcoming audits and potential financial penalties for failure to implement the provisions correctly.
In this brief, we provide a comprehensive review of the IFR, including which states and populations are subject to the new requirement, how individuals meet different exclusions or exceptions, how individuals demonstrate compliance with WRR, what data sources states must use, what verification and noncompliance processes apply, how states must target outreach to eligible or enrolled expansion adults, and what data is required of states for CMS to monitor implementation and compliance with the rule. Note that H.R. 1 and the IFR use language that is not intuitive. In this brief, we will use these “terms of art” when they have important implications for states and impacted beneficiaries.
Key Takeaways
- Fewer people will qualify as medically frail with the eleventh hour addition of the IFR’s requirement that the individual’s condition “significantly impair” their ability to work or participate in qualifying activities.
- Defining and verifying that an individual’s condition significantly impairs their ability to comply with WRRs will place an enormous administrative burden on individuals, health care providers, health plans, and states leading to more paperwork that must be processed manually.
- While the law outlines several categories of individuals excluded from WRRs (called Specified Excluded Individuals), under the IFR, some types of exclusions – most notably medical frailty – will be more difficult to verify than others.
- With critical definitions up to the states, such as what documentation is sufficient to verify medical frailty or other WRR exclusions when documentation is not reasonably available – individuals with the same circumstances could be treated differently depending on where they live.
- The added burden of implementing medical frailty requirements and other unexpected changes in the IFR sets back progress the states had made in planning, making system and policy changes, and conducting outreach.
- The burden on states is untenable. The initial 18-month implementation timeframe established by H.R. 1 was unreasonable; the IFR makes it even more unrealistic for already-overwhelmed Medicaid agencies to be ready to roll out these major policy changes by the end of 2026 without chaos and confusion.
States that Must Implement Work Reporting Requirements
(§ 435.551)
States that cover adults through the ACA Medicaid Expansion or through certain waivers that provide Minimum Essential Coverage (MEC) must implement procedures to require those adults to demonstrate compliance with federal work reporting requirements (unless the adult qualifies for an exclusion or exception, discussed below). Hereafter – “expansion adult” refers to adults enrolled in ACA expansion states and applicable waiver states.
- ACA expansion states: WRRs are required in the 41 states (including D.C.) that have expanded Medicaid to adults through the ACA. These states offer Medicaid to non-disabled adults who are not eligible for other categories of coverage (e.g., Section 1931 low-income parent or pregnant individual). These individuals are eligible under Section 1902(a)(10)(A)(i)(VIII), also known as Group VIII.
- Applicable waiver states: WRRs also apply to states that have expanded Medicaid through large Section 1115(a)(2) demonstrations or have a Section 1115(a)(2) demonstration providing MEC to targeted adult populations.1Georgia and Wisconsin are two states that have partially expanded Medicaid through a Section 1115(a)(2) waiver and offer coverage to a subset of adults up to 100% federal poverty level. While it was commonly understood that Georgia and Wisconsin would be subject to WRRs, the IFR notes that additional section 1115(a)(2) waiver populations and/or additional states could be subject to WRRs (91 Fed. Reg. 33353). In the preamble, CMS states that it is “engaged in a systemic review and analysis of approved section 1115(a)(2) expenditure authority” to identify demonstrations covering individuals who otherwise would be subject to WRR (91 Fed. Reg. 33354). See text box below.
CMS extends WRRs to more states and specific Section 1115(a)(2) waiver populations. After publication of the rule, CMS released a slide deck reporting that “to date” it had identified eight states – including Georgia and Wisconsin along with, more surprisingly, Hawaii, Massachusetts, New York, Oregon, Tennessee, and Utah – that must apply WRRs to 13 specific section 1115(a)(2) waiver populations. The idea is that some 1115(a)(2) demonstrations offer coverage to certain sub-populations that are similar to the description of Medicaid expansion adults in H.R. 1. For example, Oregon has a section 1115(a)(2) waiver demonstration offering coverage to a tiny group: young adults (between ages 19 and26) with special health care needs with income up to 300 percent of the federal poverty line. Some of these young adults fit criteria similar to that of an expansion adult who would be subject to WRRs.
Notably, while seven of the eight states CMS identified are either Medicaid expansion or partial Medicaid expansion states, Tennessee is a non-Medicaid expansion state that had not been building its state systems in anticipation of WRRs. Tennessee has a Section 1115(a)(2) waiver demonstration (TennCare III) that offers coverage to parents and caretaker relatives with income above the income standard in the Medicaid State Plan and up to a maximum level of 100 percent of the federal poverty line. In Oregon, Tennessee, and several other states, the administrative effort and cost to apply WRRs makes little sense because the demonstrations are small and largely include populations that are, by definition, compliant or excluded from the WRRs, such as individuals with medical frailty or individuals with household monthly income at or above $580 (see below for discussion of the $580 monthly income proxy in the IFR).
Since publication of the rule and accompanying slide deck, CMS has been working with at least some of the states with small, targeted Section 1115(a)(2)demonstrations to assess whether some kind of exception might be allowed for those demonstration populations.
Good Faith Effort Exemption (§ 435.560)
Under H.R. 1, in Section 1902(xx)(11) of the Social Security Act, the Secretary may temporarily exempt a state from meeting the January 1, 2027 implementation date. However, the IFR makes it clear that states cannot count on having this flexibility. Under the IFR, states must send a request that includes actions taken by the state toward implementation; significant barriers and challenges encountered; the state’s detailed plan, timelines, and milestones to achieve full implementation; and any exigent circumstances (e.g., cyber-attack or emergency). While the law provides for good faith exemptions to be granted through December 31, 2028, the rule limits an initial exemption to six months only (§ 435.560(c)). States must update the required information quarterly and show a continued good faith effort to be approved for any extension. CMS expects to issue a template for states to use in requesting the exemption. And while CMS anticipates receiving applications from ten states, they expect to approve only two (91 Fed. Reg. 33430). Thus, states are unlikely to be able to count on a good faith exemption to delay implementation even though the IFR adds new requirements and deviates from prior CMS guidance to states.
Populations Subject to or Excluded/Excepted From Work Reporting Requirements (§ 435.551)
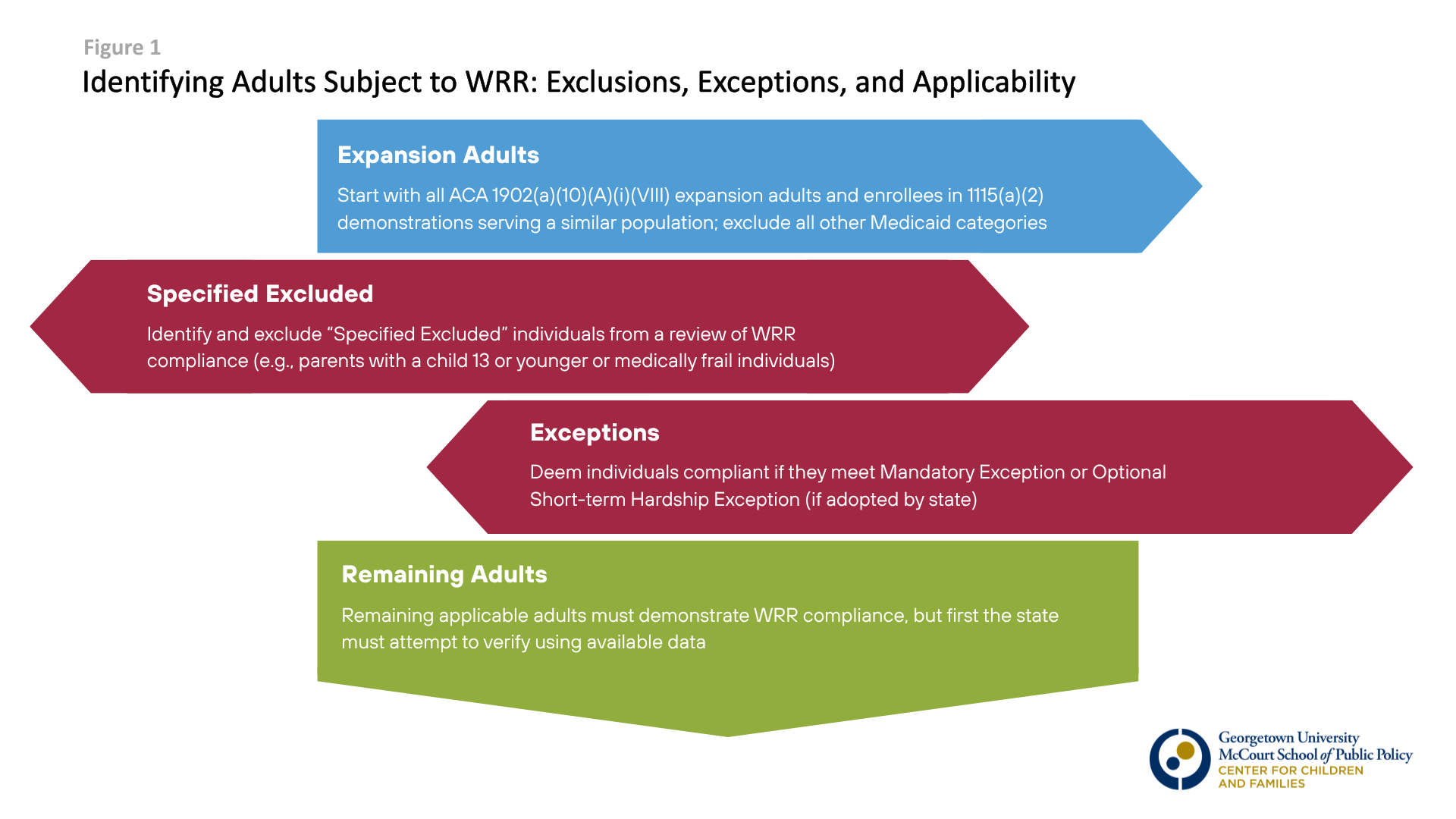
- Expansion Adults: Adults ages 19-64 eligible for or enrolled in Medicaid coverage as a Group VIII expansion adult or applicable waiver program are subject to WRRs. Individuals eligible for other Medicaid groups – such as pregnancy Medicaid coverage, Section 1931 parent/caretakers, individuals up to age 20 or 21 enrolled in Medicaid at state option as a poverty level child, or individuals with disabilities – are not subject to WRRs. (Learn more here about Medicaid for Section 1931 parents/caretakers and the income eligibility threshold in each state.)
- Within the group of expansion adults, some must demonstrate compliance with WRR (“applicable individuals”), while others are not subject to WRR (“Specified Excluded individuals”) and another group must be deemed compliant (“excepted”) because they qualify for a mandatory exception or an optional short-term hardship exception. These terms are confusing but there are important implementation ramifications. The IFR describes these groups as follows:
- “Specified Excluded Individuals” are not included in the definition of an applicable individual and are not subject to WRR when applying or renewing coverage (§ 435.554). H.R. 1 outlines nine categories of individuals – referred to as Specified Excluded individuals – who are explicitly not subject to WRRs. If an expansion adult qualifies as Specified Excluded, states may not evaluate the individual for compliance with work, school, or other community engagement hours at application, renewal, or in between renewal periods. States are expected to identify people that have Specified Excluded status first and eliminate these adults from a compliance review. The state’s determination of whether an individual is Specified Excluded is based on the individual’s circumstances in the month of application or renewal. The Specified Excluded categories, including medical frailty, are discussed in detail below.
- Expansion adults who do not have Specified Excluded status but who qualify for a “Mandatory Exception” must be automatically deemed to have demonstrated compliance by the state (§ 435.553). Not being subject to WRRs (Specified Excluded) and being automatically deemed compliant with WRRs (Mandatory Excepted) may seem like the same thing. However, unlike Specified Excluded individuals, the state’s determination of whether an individual qualifies for an exception is based on the previous month or months, called the “lookback” period. The Mandatory Exceptions are for people who are expansion adults in the month of application or renewal, but would not have been subject to WRRs during the lookback period (e.g., in the lookback period, they were under 19, entitled to or enrolled in Medicare or another Medicaid category; Specified Excluded; or an inmate of a public institution). By using a lookback period for the Mandatory Exception, rather than the current month, these individuals will be deemed compliant with WRRs once, but will have to demonstrate compliance at the next semi-annual renewal. More details on the Mandatory Exceptions are described below.
- Additional expansion adults will be deemed compliant with WRR in states that adopt the “Optional Exception for Short-Term Hardship Events” (§ 435.555). H.R. 1 gives states the option to adopt an exception for four temporary short-term hardship events, such as adults living in counties facing national emergency or disaster, although the length of the exception will vary. Similar to the Mandatory Exception, the state’s determination of whether an expansion adult qualifies for a short-term hardship event exception is based on the previous month or months (the lookback period). If an adult qualifies for a short term hardship event exception, they are deemed compliant with WRR and have a temporary reprieve from demonstrating compliance until the next semi-annual renewal or compliance check. The Short-Term Hardship Events Exception is discussed in detail below.
- The remainder of expansion adults are “applicable individuals” who must demonstrate compliance through work or qualifying activities (§ 435.551). While these individuals must demonstrate compliance, states must first attempt to verify compliance using data available to the state before requesting information from the individual (called the ex parte process). The verification process is described in detail below.
One key distinction between excluded and excepted is based on when the status is verified – in the month of application or renewal or during a lookback period prior to the month of application or renewal. The state evaluates if an individual is Specified Excluded or not in the month of application or renewal. For example, a parent with a five-year-old at application or renewal can be automatically excluded under the Specified Excluded category for parents with children 13 and younger. In contrast, for those who do not fit a Specified Excluded category and are applicable individuals at time of application or renewal, the state evaluates data in the lookback month(s) to determine if the individual meets criteria for a Mandatory Exception or Short-term Hardship Event Exception. For new applicants, the lookback period is the preceding month (or 3 months in states that adopt a 3-month lookback at application). For current enrollees, the lookback period may be any month since the last renewal (or since the last compliance check in states that adopt more frequent compliance reviews).
The examples below illustrate how the lookback period interacts with Exceptions and Specified Excluded status.

Qualifying for an Exclusion or Exception
Regardless of whether the individual is excluded, excepted, or required to demonstrate compliance with WRRs, the state’s process for assessing the individual’s status is largely the same: the state must first check available data sources without requesting information from the applicant or enrollee (also known as an “ex parte” process), request documentation only if data are not available, and accept other information if documentation if not reasonably available (§ 435.557), with some limitations. More details on specific steps for assessing compliance with or exclusion from WRRs are discussed in the next section. However, since the IFR sets out distinct – and sometimes more burdensome – verification requirements for certain Specific Excluded categories, the following section includes, where applicable, steps that states and individuals must take to verify Specific Excluded status.
Specified Excluded Individuals (§ 435.554)
As noted, Specified Excluded Individuals are not subject to WRR, but some types of exclusions within this category – most notably medical frailty – will be more difficult to verify than others. In this section, we’ll discuss the different types of Specified Excluded individuals and how states must verify the exclusion. Some exclusions, such as a parent with a child age 13 and younger, should be clear based on the application or case record. Other exclusions, particularly for people who are medically frail, may be challenging for states to verify without requesting additional information. This is a consequence of the IFR requiring that an underlying medical condition significantly impair an individual’s ability to comply with WRRs. If the state cannot confirm compliance through cross-program or other reliable data, the state must request documentation from the individual according to the verification rules at § 435.557(b), described in detail below. If documentation is not reasonably available, the state must have a process to accept other information sufficient to verify the individual’s eligibility for the exclusion.
- Former foster youth (§ 435.554(c)(1)). The Former Foster Care Child (FFCC) is a relatively new mandatory category of coverage that was intended to provide continuing access to Medicaid coverage for foster youth as they transition to adult independence. This mandatory category of coverage recognizes that foster youth don’t have families to fall back on like young adults who are eligible under the ACA to stay on their parent’s group health insurance plan up to age 26. It includes young adults under the age of 26 who were in foster care, enrolled in Medicaid, and exited foster care without an adoption or a permanent placement. The rule clarifies that the Specified Exclusion applies to all former foster youth regardless of the state where they were in foster care.
Verification. States currently collect information to determine FFCC eligibility at application and renewal. Once identified, the young adult is automatically verified on an ex parte basis until age 26, although the individual must continue to reside in the state where they are enrolled. Additionally, former foster youth who had been in foster care in another state could be enrolled in adult expansion or an applicable waiver program. Thus, the rule instructs states to use existing data in their eligibility systems (or additional screening questions if needed) to identify expansion adults who meet criteria for eligibility as a ‘former foster care child,’ and if eligible, move them into the FFCC group. CMS expects very few FFCC individuals in the Medicaid expansion group because states already screen for FFCC eligibility. - American Indians and Alaska Natives (AI/AN) (§ 435.554(c)(2)). Medicaid statute and regulations have several provisions that apply specifically to AI/AN because of the unique Federal Trust Responsibility to provide health care to AI/AN. Through reference to existing federal laws, H.R. 1 defines Specified Excluded to include individuals who are American Indian, Alaska Native, or those otherwise eligible for health services through the Indian Health Service. In the IFR, CMS notes that it has previously issued regulations to define ‘‘Indian’’ at 447.51 to implement various Medicaid premium and cost sharing protections for AI/AN. The existing definition at § 447.51 incorporates each of the specific groups listed in H.R. 1; therefore, the IFR adopts the existing definition of ‘‘Indian’’ at § 447.51 to apply to this WRR exclusion.
Verification. CMS expects states to be able to use information available to them in their eligibility systems because the state already collects information about AI/AN status for purposes of implementing Medicaid and CHIP premium and cost sharing protections and other provisions. AI/AN status is verified through official tribal enrollment and documents issued by a federally recognized tribe or the Bureau of Indian Affairs. Once identified as AI/AN, this is a permanent exclusion that does not need to be reverified. - Parents, guardians, caretaker relatives, or family caregivers (§ 435.554(c)(3)). The IFR covers a broad range of caregiving scenarios and arrangements to specifically exclude parents, guardians, caretaker relatives, or family caregivers of a dependent children age 13 and younger or of a disabled individual. The IFR defines each of the terms used in this exclusion – some of which already exist in Medicaid law and others that have not been defined previously for Medicaid policy.The IFR also clarifies that multiple caregivers in a single household may qualify for the exclusion (e.g., two adults caring for an elderly grandparent who lives with them). Specific definitions include:
- Dependent child is a child age 13 or younger and relies on another individual for care. The child does not need to be a tax dependent or living with the parent or caregiver.
- Disabled individual is defined – for the first time in the Medicaid context – as an individual who meets the broad definition of disability under the Americans with Disabilities Act (ADA) at 28 CFR 35.108. This includes an individual of any age– such as an elderly parent, grandparent, teen, or adult child – who requires assistance in performing activities of daily living (ADLs), such as bathing, toileting, dressing, eating, caring for oneself, walking, standing, among other life activities. The IFR clarifies that the disabled individual does not need to be eligible for Medicaid or other federal programs based on disability.
- Parent is defined as an individual with legal status of mother or father, including by adoption, who provides “some level of care” to the dependent child or disabled individual. Living with the person is not required.
- Guardian is an adult appointed by a court to care for and make personal decisions (not just financial decisions) for a dependent child or disabled individual who cannot care for themselves.
- Caretaker relative is an existing Medicaid term (§§ 435.110 and 435.4) used for determining eligibility for the Section 1931 Parent/Caretaker Relative category. The IFR adopts the current definition, pointing out that states are already familiar with applying it. Caretaker relative includes a parent or other relative (related by blood, adoption, or marriage) living with a dependent child, who assumes primary responsibility for the dependent child’s care. The spouse of a parent or caretaker relative remains qualified as a caretaker relative even after the marriage is terminated by divorce or death of one parent, as long as the spouse still lives with the child.
- Some states have expanded the caretaker relative beyond the federal definition for purposes of 1931 Parent/Caretaker Relative Medicaid eligibility – such as adding half-blood relatives or a domestic partner of the parent or other caretaker relative. If a state has added adults as caretaker relatives for purposes of 1931 Parent/Caretaker Relative eligibility, it must use that definition. This alignment simplifies state administration of this exclusion.
- Family caregiver is an adult family member or other individual who has a significant relationship with, and who provides care within a broad range of assistance to, a dependent child or a disabled individual. Family caregiver was not previously defined in Medicaid law; H.R. 1 introduces the term by reference to the RAISE Caregivers Act, a 2018 federal law that is specific to adults caring for “an individual with a chronic or other health condition, disability, or functional limitation.” For the purposes of the Medicaid WRRs, the IFR applies family caregiver to a broader cohort of care recipients: the care recipient can be a disabled individual or a child age 13 and younger.
- The new application of family caregiver in the Medicaid context may have many implications. Beyond the clearer examples of a husband caring for his wife with debilitating cancer, family caregiver could also refer to an aunt who cares for her niece during the day while the rest of the family is outside the home (the aunt is not a caretaker relative because she does not assume primary responsibility for the child). Inclusion of family caregiver may also open opportunities for more child care providers – including home-based child care situations – to qualify under the family caregiver exclusion.
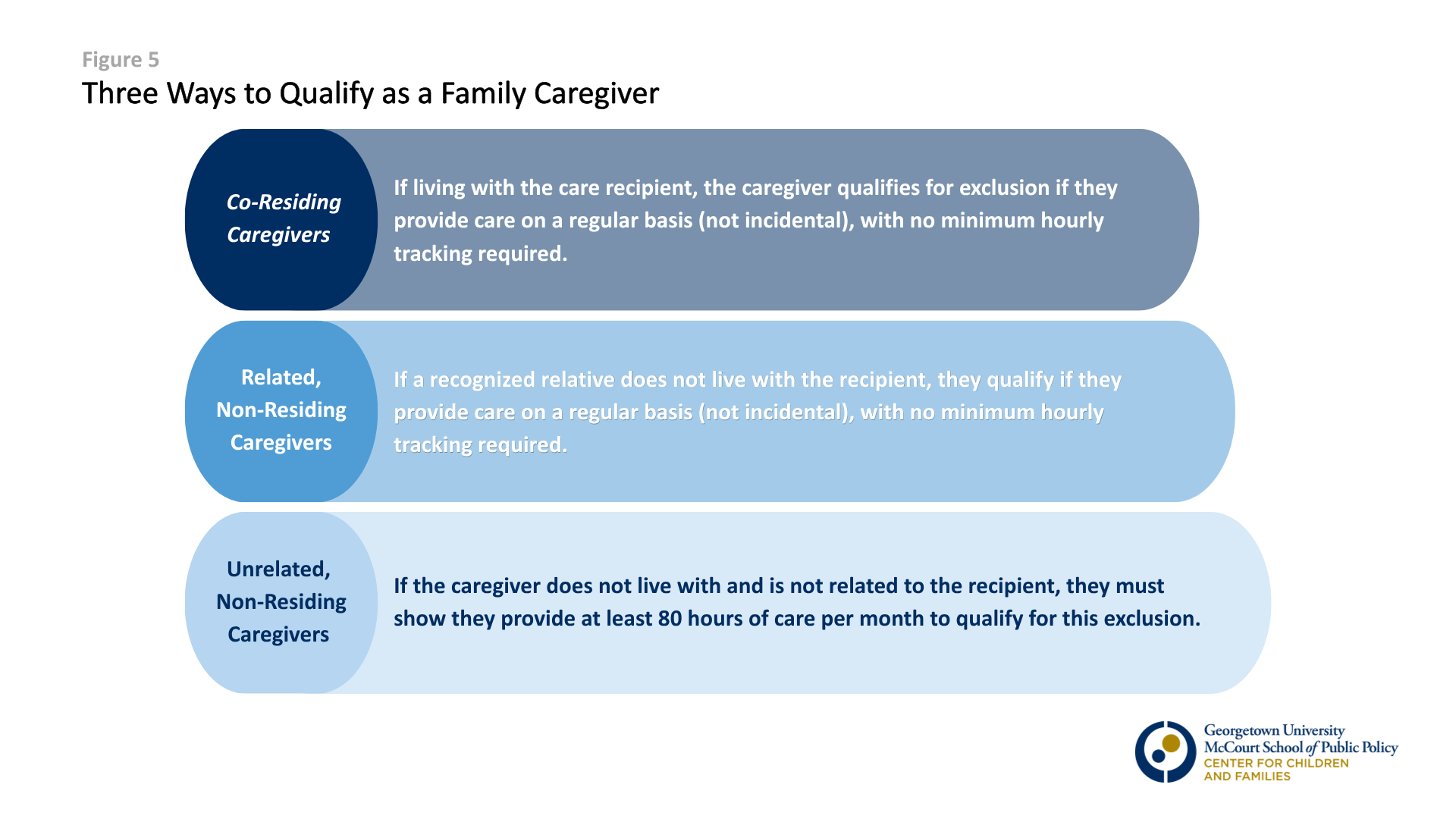
To qualify as family caregiver, the caregiver and care recipient must have a “significant relationship.” The IFR further defines a “significant relationship” by describing three caregiving situations, requiring the individual to meet at least one to qualify as a family caregiver. The scenarios cover a wide range of potential caregiving arrangements and will likely reduce the need for states to do case-by-case, subjective assessments of what constitutes “significant” relationship. See Figure 4.
Verification. States likely have information, collected at application, to verify whether an individual is a parent, guardian, or caretaker relative of a child 13 and younger. The bigger challenge – for both states and the enrollee – will be verifying caregiving relationships (and caregiving hours, if needed). There is often little to no documentation showing that an adult cares for an elderly parent, or an aunt cares for her niece on a regular basis, or an adult cares for a neighbor who is disabled (80+ hours). In 2027, the state may accept information, such as self-attestation. But, beginning January 1, 2028, when data sources available to the state do not provide necessary information, the state must require documentation whenever it is reasonably available. If documentation is not reasonably available – and in many cases, there is no documentation of informal caregiving arrangements – the state must establish a process for accepting information sufficient to verify the exclusion.
The IFR specifically uses family caregivers as an example of a situation in which it is likely that documentation is not reasonably available and requires states to take this into consideration and not deny or disenroll individuals in this or similar situations. (91 Fed. Reg. 33395).2
- Parents compliant with TANF work reporting requirements (§ 435.554(c)(6)). This exclusion applies to individuals who receive TANF benefits and are currently in compliance with their state’s specific TANF work requirements. CMS notes in the preamble that many potentially applicable individuals who receive TANF will meet other specified exclusions, such as those for parent, guardian, or caretaker relative of a child 13 and younger. In those cases, the state should exclude the parent with a young child without needing to check TANF data.
Verification. Two-thirds (36) of states have eligibility systems with Medicaid, SNAP, and TANF integrated, which allows Medicaid agencies to easily access cross-program data. If an individual meets TANF work requirements, the individual is a Specified Excluded Individual for Medicaid WWRs. If a state does not yet have the means to obtain TANF work requirement compliance information, it must establish a process to obtain information from the TANF agency or eligibility system. In the preamble, CMS notes that state Medicaid agencies should work closely with the agency that administers TANF to determine which individuals are eligible for this TANF-based Medicaid WRR exclusion, and states “should not rely on or require reporting from the individual.” (91 Fed. Reg. 33377). - Individuals receiving SNAP benefits who are not exempt from SNAP work requirements (§ 435.554(c)(7)). This exclusion applies only to individuals who are subject to SNAP work requirements. If an individual receiving SNAP is considered an able-bodied adult, SNAP benefits are severely limited to three months in a three year period, unless they meet SNAP work requirements. The rule clarifies that states are not required to independently confirm that the individual is actively completing SNAP work requirements. Simply verifying that the individual is subject to (not exempt from) SNAP work rules and in a household receiving SNAP is sufficient to trigger the exclusion from Medicaid WRRs.
Verification. Two pieces of information are needed to verify the SNAP exclusion: (1) the household’s eligibility for food assistance, and (2) the individual’s SNAP work requirement exemption status. As mentioned above, states have integrated eligibility systems and can access SNAP cross-program data as a reliable source of information. If a state does not yet have the means to obtain SNAP data, it must establish a process to obtain information from the SNAP agency or eligibility system. In the preamble, CMS notes that state Medicaid agencies should work closely with the agency that administers SNAP to determine which individuals are eligible for this SNAP-based Medicaid WRR exclusion (91 Fed. Reg. 33377); but CMS does not explicitly clarify, as it does for the TANF-based Medicaid WRR exclusion, that states should not rely on or require reporting from the individual. - Veterans who are totally disabled, either temporarily or permanently (§ 435.554(c)(4)). The disability must be service-connected and rated at total (100%) disability from the Department of Veterans Affairs (VA). This explicitly includes veterans receiving compensation via Total Disability based on Individual Unemployability determinations.
Verification. If a permanent total rating is identified, it does not need to be reviewed again. Otherwise, states must reverify a veteran’s temporary total disability status at least once every 12 months. States may reverify temporary total disability status at each renewal (every six months), but not at checks between renewals. Documentation from the VA is required. If a state does not already have connection to VA disability data, the state must request documentation from the individual showing the veteran’s permanent or temporary disability rating of 100%.- CMS notes the future availability of a Federal Data Services “Hub” that aims to offer states access to federal data sources, such as verified student enrollment records or VA disability files. If VA data becomes available to states through the Hub, states must establish a connection to the Hub within 12 months of its availability (See 91 Fed. Reg. 33405 and § 435.557(e)).
- CMS notes the future availability of a Federal Data Services “Hub” that aims to offer states access to federal data sources, such as verified student enrollment records or VA disability files. If VA data becomes available to states through the Hub, states must establish a connection to the Hub within 12 months of its availability (See 91 Fed. Reg. 33405 and § 435.557(e)).
- Active participation in a drug addiction or alcohol treatment and rehabilitation program (§ 435.554(c)(8)). Programs offered by a private, non-profit organization or publicly-operated community mental health center, as defined by the Food and Nutrition Act of 2008, qualify. The rule gives states the option to add a minimum time commitment – requiring a certain number of hours per week or days of treatment – before an individual can qualify for this exclusion. This exclusion will likely cover a narrow group of people with substance use disorders since the vast majority of people with substance use disorders do not receive treatment. (See section below for how people with substance use disorder may qualify as medically frail, with limitations).
Verification. States must attempt to verify participation in drug addiction or alcohol treatment and rehabilitation programs using adjudicated claims, payment and encounter data, and other relevant information available to the state. See verification steps below for when states may or must require documentation, and when self-attestation may be acceptable (§ 435.557(b)). - Inmates of public institutions (§ 435.554(c)(9)). The rule adopts the existing Medicaid definition of inmate of a public institution at § 435.1010, which includes individuals currently held involuntarily in custody within a state or federal prison, local jail, detention facility or other penal settings. While in custody, Medicaid services are generally limited to inpatient care. Some states have approved reentry waivers that allow Medicaid coverage of certain services in the three months prior to release. In these cases, status as a Specified Excluded Individual qualifies them for an exclusion from WRR.
Verification. Most states are already in the process of establishing data connections with corrections facilities to implement rules to suspend coverage upon incarceration and to resume Medicaid if inpatient care is needed and upon release. These same connections can be used to identify individuals who are currently incarcerated. If a state has established these data connections, verification can be processed on an ex parte basis without requesting information from the enrollee. - Pregnant or Postpartum (§ 435.554(c)(10)). Those who are pregnant when enrolling in Medicaid are generally enrolled in the pregnancy Medicaid category, which is not subject to WRRs. But individuals in the adult expansion group may become pregnant after enrolling. In general, states are not required to move these individuals to the pregnancy category, but they should be considered Specified Excluded for the duration of their pregnancy and their postpartum coverage period. All states, except Arkansas, provide 12 months of postpartum Medicaid coverage.
Verification. States must accept an attestation of pregnancy or entitlement to postpartum Medicaid unless the state has information inconsistent with the attestation. Individuals can report pregnancy when they apply, as a change in circumstances after enrollment, or at renewal – and states should use this information in their eligibility systems to determine Specified Excluded status. In addition, at renewal or where a state conducts more frequent verifications, states may use claims data, encounter data, health records, or other reliable information available to the state when determining if a previously applicable individual is now newly excluded.- States may want to require health plans to provide information once pregnancy is identified for Medicaid expansion members so that the state system can be updated with data from a reliable source.
Special Rules for Medically Frail (§§ 435.554(c)(5), 435.557(f))
Under H.R. 1, Specified Excluded individuals who are explicitly not subject to WRRs include individuals who are “medically frail or otherwise [have] special medical needs”(Section 1902(9)(A)(ii)(V) of the Social Security Act). While the statute outlines five categories of qualifying health conditions to be considered medically frail (see below), the IFR significantly narrows who actually qualifies for this exclusion.
First, the IFR narrows the definition of medical frailty to individuals who can show their health condition “significantly impairs the individual’s ability to comply” with WRRs. Second, the IFR imposes rigorous new verification rules specific to medical frailty, including heavy restrictions on self-attestation. Combined, these changes increase operational challenges and potential costs for states to implement and will create new barriers for vulnerable adults, putting more adults at risk of losing coverage – especially those with serious medical conditions. This section offers details on the new significant impairment requirement and verification rules in the IFR for this exclusion.
In late June 2026, 25 states plus the District of Columbia filed a complaint (Commonwealth of Massachusetts et al. v. Oz et al.) along with a motion for preliminary injunction in the U.S. District Court for the District of Massachusetts arguing that provisions in the IFR violate the Administrative Procedure Act as contrary to law and arbitrary and capricious, among other claims. There are a number of provisions at issue in the complaint. Notably, the plaintiff states allege that the IFR impermissibly limits the medically frail exclusion by creating a new significant impairment standard; departs substantially from the text of H.R. 1 and from direct guidance CMS issued to state Medicaid officials since the fall of 2025; and offers unworkable methods for states to comply. The case is ongoing at the time of publication of this Explainer.
The IFR Adds a Significant Impairment Requirement:
- The IFR makes it far more difficult to qualify as “medically frail” by adding a significant impairment requirement not stipulated in law. To be considered medically frail under H.R. 1, an individual must have a qualifying health condition within one of five categories: (1) blind or disabled; (2) substance use disorder; (3) disabling mental disorder; (4) physical, intellectual, or developmental disability that significantly impairs the ability to perform one or more Activities of Daily Living (ADLs); and (5) serious or complex medical conditions. Under the IFR, however, it’s not enough for an individual to have a qualifying health condition, they must also demonstrate that the condition significantly impairs their ability to work or participate in qualifying activities (§ 435.554(c)(5)).This “significant impairment” standard, not stipulated in H.R. 1 or used in preexisting Medicaid policy, will increase administrative burden on individuals, providers, and states to prove medically frail status. Narrowing the definition surprised states, many of which had already started creating medically frail definitions and diagnostic code lists based on informal guidance from CMS that followed current policy and the definition used in H.R. 1.
- While the IFR uses the same five categories of qualifying health conditions as H.R. 1, it makes several changes to the definitions of these categories and does not allow states to designate other medically frail individuals for WRRs outside of these five categories (See § 435.554(c)(5)(i)(A) – (E)).
- (1) Blind or disabled.
H.R. 1 and the IFR directly reference Social Security Act (SSA) Section 1614 to define “blind or disabled” for the purpose of medical frailty. Of note, the definition of “disabled” for medical frailty is more stringent than the way the IFR applies disability in other areas of WRRs. For example, as described above, an adult may be Specified Excluded as a family caregiver caring for a “disabled individual,” with disabled broadly defined using the Americans with Disability Act (ADA) definition of requiring assistance in activities of daily living (ADLs), such as bathing, toileting, dressing, eating, walking, standing, among other life activities. Here, since disabled is tied to Section 1614 of the SSA – which is the definition used for purposes of Supplemental Security Income (SSI) determinations – disabled for medical frailty is narrower and means a person is “unable to engage in any substantial gainful activity by reason of any medically determinable physical or mental impairment which can be expected to result in death or which has lasted or can be expected to last for a continuous period of not less than twelve months.” (See 91 Fed. Reg. 33374). - (2) Substance use disorder (SUD).
This category applies to individuals with an SUD regardless of whether they are participating in a drug or alcohol treatment program (individuals in active drug or alcohol treatment can qualify as a Specified Excluded Individual, described above). Under H.R. 1, any SUD should qualify because Congress did not include any additional conditions on this exclusion. However, the IFR limits the definition to a subset of people with SUDs: an individual “with a substance use disorder, excluding an individual in stable recovery (which means, an individual who is in recovery for 5 or more years).” (§ 435.554(c)(5)(B)). While those who are not yet in “stable recovery” may meet medical frailty criteria, those who have been in recovery for 5 or more years likely will not according to the IFR. CMS does not specify how to determine when recovery begins. - (3) Disabling mental disorder.
CMS declined to define “disabling mental disorder” in the IFR, stating that it would be difficult to set a single standard. CMS notes that three resources are commonly used to define and classify disabling mental disorders: the Interdepartmental Serious Mental Illness Coordinating Committee (ISMICC), the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), and International Classification of Diseases and Related Health Problems, Tenth Revision (ICD–10).3 Without requiring a certain approach, CMS offers that “[s]tates may find the ISMICC, DSM–5, and ICD– 10 to be useful resources for setting criteria to identify individuals with disabling mental disorders.” (91 Fed. Reg. 33375). - (4) A physical, intellectual, or developmental disability.
CMS also declined to define physical, intellectual, or developmental disability in the IFR, stating that a determination depends on the individual’s functional status and the severity of the condition. The IFR does specify that the disability must impair the individual’s ability to perform one or more ADLs (e.g., such as bathing, toileting, dressing, eating, getting in and out of bed or a chair, walking). Disabilities could be temporary or permanent. If the disability is permanent, the state should not reverify those conditions. The IFR specifically excludes Instrumental Activities of Daily Living (IADLs) (such as cooking, cleaning, transportation, laundry, and managing finances) from the definition. The exclusion of IADLs differs from other areas of Medicaid policy, such as eligibility for Home and Community Based (HCBS) services, where a person may qualify if the disability impairs the person’s ability to perform IADLs. - (5) Serious or complex medical condition.
The IFR implements a long list of criteria for “serious or complex medical condition” based on a 1999 Institute of Medicine report, “A serious or complex medical condition is a medical condition that is life threatening, seriously disabling without necessarily being life threatening, causing significant pain or discomfort that can cause serious interruptions to life activities, requiring major time or effort commitment from caregivers for a substantial period of time, requiring frequent monitoring, associated with severe consequences or negative consequences for someone else, affecting multiple organ systems, requiring management to tight physiological parameters, requiring coordination of multiple specialties, requiring treatment that carries a risk of serious complications, or requiring adjustment in nonmedical environments” (§ 435.554(c)(5)(i)(E)).
- (1) Blind or disabled.
- Although states are required to determine whether a medically frail individual has “significant impairment,” the IFR does not establish a “significant impairment” standard.The IFR requires states to develop a list of diagnostic codes and use other claims or encounter data to identify individuals who might potentially be medically frail (§ 435.554(c)(5)(ii)). However, due to the “significant impairment” standard in the definition, a diagnosis alone may not be enough for an individual to be considered medically frail and qualify for Specified Excluded status.
Operationally, this will be extremely challenging for states, as they may be unable to solely rely on a data match to a list of qualifying diagnoses or types of treatment. Nebraska, which is already implementing WRRs, was planning such an approach with a long list of medical conditions but is now revisiting this question.
Ultimately, states may need to make an individualized assessment that an individual’s qualifying condition significantly impairs their ability to work or participate in another activity to comply with the WRRs. Even if states can supplement diagnosis information with claims or encounter data, this data will speak to clinical acuity and not necessarily ability to do 80 hours of work per month.- The IFR doesn’t provide the guidance states need to implement this “significant impairment” standard, but it makes clear that CMS may audit states, including through the Payment Error Rate Measurement program (PERM), to assess implementation of the medically frail definition in compliance with the IFR. This could potentially push states to over-verify eligibility in a way that leads to inappropriate denials or disenrollments that result in people with serious medical conditions losing access to care.
The IFR Imposes New Verification Rules Specific to Medical Frailty:
- While leaving the definition of “significant impairment” to the states, the IFR adds specific steps for verifying medical frailty that will be challenging and potentially costly for states to implement (§ 435.557(f)). H.R. 1 does not reflect a statutory intent to create different, more restrictive verification processes for medical frailty as opposed to other Specified Excluded categories.
- In 2027, if a state is unable to verify medical frailty electronically, the state may require documentation or accept a statement or other information (§ 435.557(f)(1)(i)). States have the option – in calendar year 2027 only – to accept self-attestation, which is an individual’s signed declaration submitted under penalty of perjury. The information would be auditable (by the state or CMS) and must provide sufficient information, as determined by the state, to verify an applicant or enrollee is medically frail or has special health care needs.
- Starting January 1, 2028, the agency may only accept a statement or other information under the penalty of perjury once during an enrollment period (§ 435.557(f)(1)(ii)). A period of enrollment means a continuous period, without a gap, which could be much longer than the 6-month renewal period. At the individual’s next renewal, if electronic data is still not available to the state, the state must require documentation submitted by or on behalf of the individual to verify that they are medically frail or have special medical needs. Since the IFR adds that individuals must show their condition “significantly impairs” their ability to meet WRRs, states have a new challenge to decide what documentation they will accept to verify medical frailty and special medical care needs. If documentation is not reasonably available, the state must have a process to accept other information sufficient to verify the individual’s eligibility for this hardship.
- When checking data sources available to the state, states must use all adjudicated claims whether they were paid, pended, or denied, as well as encounter data, from the prior 12 months to verify medical frailty and special medical care needs (§ 435.557(f)(1)). “Adjudication” refers to the date a claim enters the state claims system, and since there is sometimes a delay between service date and adjudication, the 12-month lookback will effectively be inclusive of services that are older than 12 months. However, the impairment requirement greatly reduces the likelihood that states will be able to make a determination without requesting additional information or documentation from the enrollee or his/her provider.
- After the state has verified medical frailty or special medical needs through data or documentation, the state must re-verify this status at least every 12 months (§ 435.557(f)(1)(iii)). H.R. 1 includes a new mandate that expansion adults must renew their Medicaid eligibility every six months instead of annually. Under the WRR IFR, while states conduct 6-month renewals for other Medicaid eligibility criteria, states may exclude already-verified medically frail individuals from a WWR compliance review at the 6-month renewal. Re-verifying medical frailty every 12 months (rather than six months) helps ensure enrollees’ ongoing access to health care while reducing the state’s administrative burden during six month renewals. Note this special rule applies only after the state verifies medical frailty or special medical needs through data or documentation, not self-attestation, which is a method available in 2027).
What is self-attestation?
If a state is unable to obtain information using available data, the IFR outlines when states may or must require extra documentation, and when self-attestation may be acceptable (§ 435.557(b),(c), and (f)). Self-attestation is an individual’s signed declaration submitted under penalty of perjury. It is auditable by the state or CMS and is currently used in other areas of Medicaid policy, such as attesting to pregnancy.
Mandatory Exceptions (§ 435.553)
The list of Mandatory Exceptions includes individuals who have become newly eligible as an expansion adult or no longer qualify as a Specified Excluded Individual as the result of a change in status. Individuals who qualify for a Mandatory Exception include: individuals in mandatory coverage groups under Section 1902(a)(10)(A)(i)(V-VII), under age 19, entitled or enrolled in Medicare Part A or B, incarcerated in the past three months, or a Specified Excluded individual. This list may seem confusing because these individuals are either not eligible for or enrolled in ACA expansion or an applicable waiver or are already captured as a Specified Excluded Individual and thus not subject to WRR. But, these groups do not overlap because there are key differences in how the two provisions (Mandatory Exceptions and Specified Excluded Individuals) are assessed.
There is a critical distinction in how Specified Excluded status and Mandatory Exceptions are verified, which explains how Mandatory Exceptions serve as a bridge when status changes. Specified Excluded status is based on the current month while Mandatory Exceptions are determined by a prior period. The state first assesses whether an individual is Specified Excluded or applicable individual based on the month of application or the renewal month. If the adult is an applicable individual, they must demonstrate compliance with WRR in the lookback period, unless they meet an exception during that lookback period. For current enrollees, the lookback period goes back to the last renewal (or last quarterly compliance check if adopted by the state), meaning that the change occurred at any time since the last review. However, the lookback period for new applicants is generally limited to the month prior to application, as determined by the state (a few states have adopted a 3-month lookback period for applicants). Mandatory Exceptions provide a temporary reprieve from WRR when there is a status change in a recent month or months.
Example 1: In January, Jane enrolls in Medicaid as an expansion adult who is Specified Excluded from complying with the WRR because she is a parent of a child 13 and younger. Jane’s daughter turns 14 in March. At Jane’s renewal in July, she is now an applicable individual subject to the WRR. But Jane was a Specified Excluded Individual during the lookback period which goes back to January, so she qualifies for a Mandatory Exception until her next renewal.
On the other hand, if Jane newly applied for coverage in July, Jane is an applicable individual but she does not qualify for a Mandatory Exception because the lookback at application is limited to the month of June when her daughter would have already turned 14. She would have to meet WRR through another pathway.
If Jane had newly applied in the month of April, she would have qualified for a Mandatory Exception because her daughter was 13 for part of the lookback month.
Example 2 : An 18-year-old named Jack enrolls as a child in Medicaid in January 2027. Jack turns 19 in June 2027 and is no longer eligible as a child. This is an anticipated change in circumstances that states must act on at the end of an individual’s birthday month. However, during the lookback period preceding the change, Jack was under the age of 19 and so he qualifies for a Mandatory Exception. Jack will not have to comply with WRR until his first renewal as an expansion adult in December 2027.
States should be able to automatically verify Mandatory Exceptions for individuals who were previously enrolled, as the case file should have the status recorded. Individuals who qualify for a Mandatory Exception must be deemed compliant until the next review. If ex parte data or other information reflect that an individual was Specified Excluded in the prior review but is now an applicable individual as the result of a change, the state must deem the individual as compliant. These individuals should not have to provide documentation, as the case file should have the status recorded. States should be able to verify a Mandatory Exception for most new applicants based on information provided in the application.
Optional Exception for Short-Term Hardship Events (§ 435.555)
States have the option to adopt an exception that covers four specific short-term hardship events, giving applicable individuals a temporary reprieve from demonstrating WRR compliance (§ 435.555). If an applicable individual meets the hardship event criteria, they are deemed compliant with WRRs during a given month until the next redetermination (or next quarterly compliance check if adopted by the state).
The four short-term hardship events, detailed below, are quite different and include: individuals receiving inpatient or other institutional care; individuals in a federally-declared disaster or emergency area; individuals living in counties with high unemployment rates; and individuals or their dependents who are required to travel outside their home for medical care for an extended time.
The IFR clarifies that, if a state adopts the optional exception, they must adopt all four hardship events (91 Fed. Reg. 33380). States must indicate if they are adopting the short-term hardships exception in a state plan amendment (SPA). A state’s election can be changed at any time via submission of a SPA. If adopted, the state must provide notice to applicable individuals when the state adopts or drops a short-term hardship exception (§ 435.561(b)(3)(ii) – (iv)).
- For hardship events that must be requested by an individual (rather than apply automatically, see below), the state must also provide notice to individuals about how to request an exception, a state’s decision about a request, and how to appeal. (§ 435.555(c)(2)).
- For hardship events that are county-based and automatic (see below), states must give notice to affected enrollees that a short-term hardship has become available (e.g., an emergency or disaster occurred or a high unemployment rate hardship is available), the anticipated duration or end date of the exception, and later, provide notice to affected individuals upon an anticipated expiration of the hardship event (§§ 435.555(c)(1) and 435.561(b)(3)).
States evaluate if an individual meets a short-term hardship event exception based on the lookback month(s), not the month of application or renewal, leading to illogical results. For example, individuals who received hospital or inpatient care during a month may qualify for a short-term hardship exception from WRR; but, the hospitalization would have to occur in the month preceding application or the month(s) prior to renewal. The result is many will not be able to qualify for the exception simply due to the timing of their hospitalization (see more details below).
Two of the four events must be automatically administered by the state while two will require enrollees to request the exception (§ 435.557(g)(2)). If the event is one the state must administer, it must automatically apply the exception to all affected enrollees or applicants residing in the specific county or counties without requesting information from the individuals. The state must send a notice to all individuals affected, noting the duration of the hardship. Under the statute and the IFR, a short-term hardship event exists if an enrollee, for all or part of a month in the lookback, meets one of the following criteria:
Hardship Events Automatically Administered by the State
- Federally-declared emergency or disaster (§ 435.555 (d)(2)). The individual lives in an area where a federal emergency or disaster has been declared under either the National Emergencies Act (NEA) or the Robert Stafford Disaster and Emergency Assistance Act. The state must notify CMS of its plan to activate the disaster or emergency hardship. Slightly different criteria apply if the event is a federally-declared disaster or emergency.4 Of note, for an NEA emergency hardship, states must show to CMS that the emergency “affects the ability of individuals” in the local area to demonstrate WRR (§ 435.555 (d)(2)(iii)). States must store and be able to produce records supporting verification of the federally-declared emergency or disaster hardship upon request, for an audit or other review.
- High local unemployment (§ 435.555 (d)(3)). The individual lives in a county or equivalent unit of local government with an unemployment rate of at least 8 percent or 1.5 times the national unemployment rate (whichever is lower). Although not specified in H.R. 1, the IFR clarifies that the Bureau of Labor Statistics (BLS) is the primary data source, but states have some flexibility. CMS notes that BLS data is commonly based on data from prior months, and a state might believe that the available BLS information does not reflect recent circumstances or widespread layoffs affecting a particular county. To account for this situation, the state may submit more recent preliminary data from a reliable source, such as a state labor department, reflecting the unemployment rate in a county. States must seek CMS approval to effectuate the high unemployment hardship. The preamble notes that states are not required to implement the unemployment-related hardship even when conditions are present in the state and a county meets the unemployment rate threshold (91 Fed. Reg. 33386).
Hardship Events that Must be Requested by the Enrollee
- Inpatient or institutional care (§ 435.555 (d)(1)). Individuals who received services in an inpatient hospital, nursing facility, intermediate care facilities for individuals with intellectual disabilities, inpatient psychiatric hospital, or other services of similar acuity, are excepted from WRRs . This may include community- and home-based services if there is evidence that the person would likely have needed institutional placement.
Verification. The state must first attempt to verify an applicable individual has received inpatient services using reliable information available to the state before requesting information from the individual. This should include adjudicated claims and encounter data for the prior 12 months. Beginning January 1, 2028, if no reliable information is available to the state, the state must require documentation if reasonably available – for example, a medical bill or admission or discharge paperwork. If documentation is not reasonably available, the state must have a process to accept other information sufficient to verify the individual’s eligibility for this hardship.
- It’s important to emphasize that this exception is determined in the lookback period, not the current month, which may produce illogical results. An uninsured individual who is hospitalized in March could not apply for Medicaid in March and qualify for this hardship exception because the exception is based on the lookback month and the event did not occur in February. If applying in April, they would qualify for the exception, but they would not qualify for retroactive coverage5for Medicaid to pay the March hospital bill unless they were compliant with WRRs in February.
- It’s important to emphasize that this exception is determined in the lookback period, not the current month, which may produce illogical results. An uninsured individual who is hospitalized in March could not apply for Medicaid in March and qualify for this hardship exception because the exception is based on the lookback month and the event did not occur in February. If applying in April, they would qualify for the exception, but they would not qualify for retroactive coverage5for Medicaid to pay the March hospital bill unless they were compliant with WRRs in February.
- Extended medical travel (§ 435.555 (d)(4)). If an applicable individual or their dependent must travel outside of their community for an extended period to receive medical services for a serious or complex medical condition not available within their community they could qualify for this exception. CMS does not define an “extended period of time.” The person may meet this hardship if the circumstances existed “for part of a month or longer.” States are not allowed to require the individual to show medical travel for a full month or longer. In addition, states have discretion to define travel “outside of their community.” A serious or complex medical condition is defined by cross reference to the new definition under medical frailty in § 435.554(c)(5)(i)(E).
If the individual’s dependent is receiving medical care, the individual can qualify if they show they took leave from employment or other community engagement activities for reasons related to the dependent’s condition or travel (e.g., taking the dependent to medical appointments to prepare for travel, conducting logistics for travel, or maintaining primary responsibility for communicating with the dependent’s medical providers). This applies even if the individual did not travel with the dependent. For purposes of this hardship event, dependent has a specific definition at § 435.555(a)(1) that may include minors and adult children, depending on the circumstances. Dependent includes a minor child living with the applicable individual or a tax dependent of an applicable individual (whether or not tax dependent is a minor child or residing with the applicable individual)
- Notably, the short-term hardship applies only for the month(s) in which the applicable individual or their dependent traveled for medical care. If an individual takes leave from work in the month before medical travel or in the month after medical travel to aid in healing or recovery, the short-term hardship would not apply in the prior or subsequent months because the individual or dependent is not traveling.
Verification. States must first use reliable information available to the states to verify the serious or complex medical condition, the receipt of medical services, and the location and dates of service – including through adjudicated or encounter data for the preceding 12 months. If the dependent traveled for medical care, the state must verify the relationship to the individual using information in the individual’s case record or the state’s eligibility system, where possible. In many cases (especially if the dependent who traveled for medical care is not covered by Medicaid), the state may not have information in its data sources. Beginning in January 2028, the state must require documentation if reasonably available, such as medical records providing the dates and location of services. If documentation is not reasonably available, the state must have a process to accept other information sufficient to verify the individual’s eligibility for this hardship.
Demonstrating Compliance
Types of Work and Qualifying Activities (§ 435.552)
Under § 435.552, an applicable individual can meet WRR for any given month by satisfying any one type or a combination of work and qualifying activities for 80 hours per month as outlined in the statute. The IFR clarifies that states must count all of the following situations to determine compliance and may not restrict participation to a narrow subset of choices.
- Qualifying work (§ 435.552(a)(1) and (b)). Demonstrating compliance with work hours includes traditional, paid work and self-employed work, as well as other work hours such as in-kind and unpaid work. Unpaid work differs from community service (below) because it can benefit a private entity or individual, such as internships or trial period work. The primary difference is that it does not need to be a direct benefit to the community through a nonprofit or public agency.
- Inclusion of unpaid work might be particularly important for informal child care providers or family caregivers that do not otherwise meet Specified Excluded criteria.For example, a person may care for their neighbor’s children in the evenings while their parents work extra shifts. An unrelated, non-residing caregiver must show 80 hours per month to meet Specified Exclusion (see above); but, informal caregiving hours below the 80-hour threshold can be counted as unpaid work hours and combined with other activities to reach the 80-hour monthly requirement.
- Inclusion of unpaid work might be particularly important for informal child care providers or family caregivers that do not otherwise meet Specified Excluded criteria.For example, a person may care for their neighbor’s children in the evenings while their parents work extra shifts. An unrelated, non-residing caregiver must show 80 hours per month to meet Specified Exclusion (see above); but, informal caregiving hours below the 80-hour threshold can be counted as unpaid work hours and combined with other activities to reach the 80-hour monthly requirement.
- Community service (§ 435.552(a)(2) and (b)). Applicable individuals may also demonstrate compliance through volunteering or unpaid work in a structured program that directly benefits the community. The program must be completed under the auspices of a public agency or non-profit organization and address a civic, public, or community need. The activity may not serve a partisan purpose. The IFR adds that for hours to count as community service, the nonprofit organization or public agency must provide oversight and have a process in place to track dates/hours. Court-ordered community service or diversion programs also count toward the required number of hours.
- Governmental work or training program (§ 435.552(a)(3) and (b)).The IFR adopts the statutory definition of work program from Food and Nutrition Act of 2008, which includes programs such as SNAP Employment and Training programs, VA training programs, and others.
- Education (§ 435.552(a)(4) and (c). An applicable individual who is enrolled at least half time in an approved educational institution can demonstrate compliance with WRRs without logging hours. Approved educational programs include institutions of higher education (colleges/universities), career and technical education programs providing secondary or postsecondary technical credentials, standard high schools, and state-approved programs preparing individuals for a high school equivalency certificate (such as a GED program). Independent study or unmonitored online test preparation does not qualify.
The IFR further clarifies that the school or institution determines whether a student is full-time, half-time, or less than half-time, and this is typically reported to the National Student Clearinghouse. Enrollment status starts on the first day of the academic term and continues through scheduled breaks. A student’s status during a winter break or summer recess is evaluated based on their enrollment status immediately prior to the break. For example, a full-time high school student who graduates on May 15 and is fully registered to begin a full-time community college program on August 21 is considered compliant during June and July. - A combination of 80 hours across work, community service, work programs, and less-than-half-time educational courses (§§ 435.552(a)(5), (d), and (e)). Applicable individuals can also demonstrate compliance with the WRR through a combination of the activities above. CMS notes that states should stop counting once an individual meets the 80-hour threshold (91 Fed. Reg. 33360). The IFR sets out a credit hour conversion standard for students who are enrolled less than half-time in educational courses – each single credit hour translates to 3 hours of educational activity per week. For technical or vocational certification programs that do not use credit hours (such as welding, cosmetology, or machining), hours are credited based on a 1-to-1 ratio of actual time spent in class, executing clinical rotations, or participating in structured lab work.
Using an Income Proxy Instead of Counting Hours (§ 435.552(f))
- States must use an income proxy based on the federal minimum wage multiplied by 80 hours (currently $580 per month) to verify compliance with WRRs (§§ 435.552(a)(6) and (f)). The monthly income proxy is the most streamlined way for states to use ex parte data to verify income and compliance with WRRs. States with higher state minimum wages may not use their state-specific rates; the federal minimum wage is the exclusive baseline for this income proxy calculation.
- The IFR confirms the use of MAGI-based household income to determine compliance with WRRs for all applicable adults in the family (§ 435.552(f)). States must apply the Modified Adjusted Gross Income (MAGI) standard to WRRs in the same way it is used for financial eligibility for Medicaid – the total household MAGI income counts toward the eligibility of all individuals in the household. Therefore, if two adults in a family have a combined household income of $580 or above, then all applicable adults in the household will be determined compliant with WRRs. By using MAGI standards that states are already familiar with, this streamlines calculation of income for WRR compliance. MAGI income includes only taxable income sources, plus a few adjustments. See Appendix A for more details on MAGI income counting rules, including taxable versus non-taxable income sources and how MAGI doesn’t treat everyone equally.
- States may convert income that is below $580 into work hours. For income below $580, the state can divide income by the federal minimum wage to convert income into work hours, which can then be used toward the combined 80 hours (see above; combination of 80 hours across work, school, community service). For example, $290 in income would convert to 40 work hours. If household income for two adults is below $580, states must use a reasonable method to allocate work hours between members of the household.
- States have two options for calculating average income for seasonal workers (§§ 435.552(a)(7) and (g)). If an individual is designated as a seasonal worker under Section 45R(d)(5)(B) of the Internal Revenue Code (such as agricultural workers or retail staff employed exclusively during holiday seasons), they meet WRRs if their average monthly household income over the preceding six months meets the $580 monthly income proxy. States may either (1) use average income for seasonal workers over the past six months or (2) count “reasonably predictable changes” in income (§ 435.603(h)(3)). If a state already uses the “reasonably predictable changes” in income approach as part of their MAGI methodology for calculating financial eligibility for Medicaid, then the state must continue to do so for determining compliance with WRRs (§ 435.552(g)). Under the reasonably predictable changes method, by prorating income over a 12-month period, seasonal fluctuations are smoothed out and may provide a more accurate assessment of average income across the year.6
- States that have not adopted the “reasonably predictable changes” methodology may want to implement the policy to more fairly distribute seasonal income over a full year.
State Processes for Assessing Compliance with or Exclusion from Work Reporting Requirements (§§ 435.556, 435.557)
States must require applicable individuals (§ 435.551) to demonstrate compliance with WRRs, or be deemed to demonstrate compliance as a mandatory exception (§ 435.553) as described above or through a short-term hardship exception (§ 435.555), in states that adopt the short-term hardship exception. But first, states must check all reliable data available to the state to identify exclusion or compliance status before requesting information from the applicant or enrollee (the “ex parte” process)(§ 435.557(b) and (c)). The state may only request information from the individual if it is unable to verify using available data, or the state has conflicting information that must be assessed (§ 435.557(a), (b), (c), and (f)).
This section describes the data sources the IFR requires states to use, the lookback periods for verifying new applicants and enrollees, and the verification steps states perform when determining an individual’s compliance with, exclusion from, or exception from WRRs.
Verification Data Sources (§ 435.557)
The IFR lists specific data sources and information that states may use for purposes of identifying Specified Excluded individuals, compliance, or deemed compliance with WRRs (§ 435.557(a)). Reliable information available to the states include, but is not limited to:
- Electronic sources that agency has determined effective;
- Information from other state or local agencies (e.g., SNAP or corrections facilities);
- Information from federal agencies available through the federal data services hub;
- Information in the state’s eligibility system and the individual’s case record;
- Payroll or income data;
- Relevant claims data adjudicated in past year;
- Encounter data from preceding 12 months;7
- Student enrollment information from colleges or other educational programs
The rule allows states to do a cost/benefit analysis when deciding whether to connect to a new data source (§ 435.557(b)(1)(ii)). The IFR allows states to determine that establishing a connection would not be effective after considering such factors as administrative costs to establish and use the data source compared to the administrative costs of processing paperwork on an ongoing basis, as well as the impact on program integrity. While the impact is still unclear, this provision may offer states an opportunity to decide against connecting to new data sources and, instead, rely more on manual, paper-based processing and documentation generated by individuals.
States are required to use the federal data services hub, which provides access to data from various federal agencies (§ 435.557(e)). The hub currently provides access to data from SSA, Internal Revenue Services, Department of Homeland Security, Treasury, and other federal agencies. CMS intends to add new data sources to help states verify certain qualifying activities for WRRs. If information from a new data source becomes available, the state must connect to the data through the hub, establish a direct connection, or implement an alternative data source within 12 months.
States must document their data sources, policies, and procedures in the state’s verification plan, which has been updated for WRR (§ 435.557(b)(iii)). The plan must include details of how the state will verify compliance or deemed compliance. CMS has released a WRR supplement to the Medicaid verification plan to collect relevant information. The verification plan and supplemental materials will likely be what CMS looks to and uses in future years to measure compliance during audit.
Lookback Periods for Verification (§§ 435.556 and 435.557(d))
Under H.R. 1, expansion adults must renew their Medicaid eligibility every six months instead of annually. With respect to WRRs, states determine how many months of WRR compliance will be required (with some limitations) for new applicants and for current enrollees. States have the option to verify compliance more frequently than every six months at renewal (i.e. quarterly checks) (§§ 435.556(a) and 435.557(d)).
- New applicants must meet WRRs in the month prior to the month of application (or up to three months prior if adopted by the state)(§ 435.556(a)(1)). States must determine compliance with WRRs for new expansion adult applicants for at least one month, but not more than three consecutive months, immediately preceding the month of application. Most states plan to look at one month prior to application.
- Unless someone qualifies as a Specified Excluded Individual, events that occur in the month of application cannot be used to verify an exception, creating a barrier particularly for those who experience a short-term hardship, such as hospitalization. This raises a paradox for individuals who apply in the same month they experience a qualifying hardship event exception, such as someone who suffers an acute medical emergency and needs inpatient treatment. The qualifying exception (inpatient treatment) is occurring in the current month, but the compliance review is based on preceding months when the qualifying condition was not yet present.
It is unclear how states and CMS will resolve this paradox that exists in both H.R. 1 and the IFR. This illogical gap between how the lookback period interacts with the hardship exception was also raised in the complaint filed by 25 states plus the District of Columbia in June 2026 asking the court to vacate and set aside specific provisions of the IFR (Commonwealth of Massachusetts et al. v. Oz et al.).
- Current enrollees must meet WRRs in one or more months since their last renewal date (or since their last review if the state adopts more frequent compliance checks) (§ 435.556(a)(2)). Most states plan to require compliance for one month since the last renewal or review. States may require compliance in multiple months since the last renewal date. If a state requires multiple months of compliance (e.g. 3-month lookback for existing enrollees), it does not need to be consecutive months. Enrollees can decide whether to demonstrate their compliance in consecutive or non-consecutive months since the last review.
- While states must renew Medicaid eligibility for expansion adults every six months, states may elect to reverify medical frailty once every 12 months (rather than every six months), but only if the state has already verified medical frailty through data or documentation as opposed to self-attestation (435.557(f)(1)(iii))). As discussed above under Special Rules for Medical Frailty, the IFR allows self-attestation submitted under penalty of perjury in 2027 and once after that; subsequently, individuals must submit documentation to corroborate medical frailty. Once met, states may reverify medical frailty every 12 months (rather than at every six-month renewal), which can reduce the administrative burden on states and medically frail enrollees and reduce the risk of inappropriate loss of coverage due to paperwork.
- The state administrative process prior to sending a renewal form or notice takes a minimum of two months, which significantly limits the period of electronic data available for review. States may only look back to the date of the most recent WRR compliance check, typically six months prior. Because the administrative process takes at least two months, states conducting renewals semi-annually would typically have a four-month compliance review period.
- Quarterly compliance checks in between semi-annual renewals dramatically restrict the amount of data available to the state – and are potentially unworkable. States have the option of more frequent checks to verify WRRs in between renewals for applicable individuals but not Specified Excluded Individuals (§ 435.557(d)). Two states (New Hampshire and Indiana) passed laws requiring both a 3-month lookback period for renewals and quarterly compliance checks. As noted above, because the administrative process takes at least two months, states conducting renewals semi-annually would typically have a four-month review period for WRR compliance. But, in states choosing quarterly compliance checks, the compliance review period would be reduced to just one month. Not only will the review period be limited, but also the availability of data will be limited because of lag time in certain reliable data sources (for example, quarterly wage reports). The chances of verifying exclusions, exceptions or compliance automatically through data sources are greatly reduced. Thus, the short review period coupled with the data lag will lead to more enrollees being required to submit proof of compliance or exclusion, creating more administrative burden and resulting in inappropriate loss of coverage. See Figure 6 below.
The two scenarios below illustrate how choosing to conduct a quarterly compliance review in between semi-annual renewals dramatically restricts the amount of data available to the state – and is potentially unworkable. There is a greater likelihood that the state will be able to confirm WRR compliance or exclusion using data from a longer review period. The administrative process requires a minimum of two months and states only look at data since the last review. Between the time required to initiate the ex parte process, review the data, provide enrollees with 30 days to respond, and send any adverse notice at least 10 days in advance, states with more frequent compliance checks will likely find this challenging and potentially unworkable.

Verification Steps (§ 435.557)
Similar to current Medicaid eligibility policy, states must first check data available to the state before requesting information from an applicant or enrollee. If a state is unable to verify using available data, the IFR outlines when states may or must require documentation, and when self-attestation may be acceptable (§ 435.557(b),(c), and (f)). In particular, the IFR outlines verification steps for 2027 only, and required verification steps starting in January 2028 and after when the rules become more stringent. In many places, the IFR lays out distinct verification requirements for certain Specified Excluded categories, including medical frailty. Those distinct rules are discussed in the Specific Excluded Individuals section above.
If information is required at renewal or to verify WRR compliance, the state must give the individual 30 days to respond (§ 435.558(a)(2)). If the individual responds with information indicating they are not eligible, or neglects to submit the information, they must be given a 10-day advance notice with appeal and fair hearing rights prior to termination (§ 435.558(d)).
- In the preamble, CMS acknowledges that a state may collect all reliable information available to the state at once (91 Fed. Reg. 33393). This approach allows a state to have both compliance- and renewal-related information available for review at one time (such as income data and information that may identify a person as Specified Excluded). States are not required to change their existing procedures to implement a specific hierarchy when checking reliable information, but they must make every effort to identify and not seek information from a Specified Excluded Individual (91 Fed. Reg. 33393). If a state has sufficient information to verify that any individual meets WRRs, but has information that suggests they are Specified Excluded, the state must enroll the individual and attempt to verify the exclusion post-enrollment (§435.557(c)(3)).
Verification Steps for States (see § 435.557(a) – (c))
- Use all reliable data sources documented according to the state’s verification plan
- Exclude all individuals who qualify as Specified Excluded Individual from WRR review
- Deem compliant individuals who qualify for a mandatory or short-term hardship exception
- Evaluate compliance with work or qualifying activities
- If reliable data is not available or the state has conflicting information, request information or documentation from the individual
- Accept documentation through all modes of communication: online, by telephone, via mail, in person, or other electronic means
- Steps for seeking information from individuals for identifying Specified Excluded individuals, exceptions, and compliance with WRRs (§ 435.557(b)) (Steps below do not apply to medical frailty, which are in 435.557(f)):
- In 2027 only: When data is not available to the state, “the agency may require documentation or accept other information.” This can be an individual’s self-attestation (i.e. auditable self-declaration)
- Starting January 2028 and after: When data is not available to the state, the state must require documentation if documentation is “reasonably available”.
- If documentation does not exist or is not reasonably available, the state must accept information other than documentation to verify an individual’s eligibility.
- States may not terminate or deny coverage solely because the individual cannot produce documentation where none exists and/or is not reasonably available.
- States have discretion to establish a process and define what information is considered “sufficient” to verify the individual’s eligibility where documentation does not exist and/or is not reasonably available. States should document their process and criteria in policy manuals and procedure handbooks for training and audit purposes.
- The requirements for verifying medical frailty are much stricter than those for other Specified Excluded Individuals or applicable individuals. In 435.557(f), the IFR has separate verification steps for verifying medical frailty, discussed above in Special Rules for Medically Frail. However, H.R. 1 does not reflect a statutory intent to create different, more restrictive verification processes for medical frailty.

Noncompliance Procedures (§ 435.558)
If the state is unable to verify compliance automatically, at application, renewal, or a more frequent check, it must provide the individual with the notice of noncompliance (§ 435.558(a)(2)). The notice must give the individual 30 days after the notice is received (notice is considered to be ‘received’ 5 days after the date on the notice) to provide information or documentation. States may not extend the 30-day notice beyond the renewal end date.
- The preamble recommends that states align the 30-day noncompliance notice with the required 30-day response time to return renewal information (91 Fed. Reg. 33411), but there are pros and cons to this approach. Under current Medicaid policy, states must give Medicaid enrollees a minimum of 30 days to respond to a renewal form; states may give enrollees more time. On one hand, aligning the 30-day response time for an enrollee to return renewal information and respond to the noncompliance notice would help a state coordinate review of WRR compliance and ongoing eligibility. However, individuals may be confused by the title of the notice of noncompliance since it implies that a decision has been made. Individuals may be best served by sequential notices; i.e., the enrollee receives the renewal notice/packet, enrollee submits required information, state reviews that information, and state sends notice of noncompliance if the information is insufficient to verify WRR compliance. On the other hand, sequential notices will also require the state to start the ex parte process a month earlier, reducing the amount of data available to the state. Sequential notices might cut down the number of noncompliance notices sent, but it would still require the cost of a second mailing. Less data means the state will be able to automatically verify fewer individuals based on the data available to the state, which adds to administrative burden for the state and individuals.
- The notice must clearly explain how the individual can demonstrate compliance or that they qualify for an exclusion or exception (§ 435.558(c)). The notice must inform the individual of the deadline and ways to submit needed information or documentation. It must also detail the consequences of noncompliance with WRRs, including losing Medicaid and ineligibility for premium tax credits to help pay for health coverage through the Health Insurance Marketplaces.8
- Individuals may reapply for coverage; and states may not put any restrictions on re-applying (§ 435.558(e)). If an individual submits the missing information or documentation within the 90-day reconsideration period, they will not need to complete a new application. However, the information is treated as a new application and the individual is subject to compliance as a new applicant.
- After considering any other basis of Medicaid eligibility, the state must deny applications or disenroll current enrollees at renewal when it is unable to verify compliance (§ 435.558(d)). For current enrollees, the state must provide written notice and fair hearing rights with a 10-day advance notice of adverse action (§ 435.558(d)(2), consistent with fair hearing rights in § 435.917).
- The IFR allows states to terminate coverage at the end of the month following the 30-day noncompliance period and after provision of written notice and fair hearing rights (§ 435.558(d)(2)(ii). This timeline could help enrollees if states experience backlogs in processing WRRs and are unable to get the written notice out immediately at the end of the 30-day noncompliance period.
Implementation Timeline (§ 435.559)
Under H.R. 1, states must implement WRRs no later than January 1, 2027, but there are outreach notice requirements that kick in prior to 2027 as described below. Very few states are implementing WRRs prior to the deadline of January 1, 2027, although it is allowed via submission of a SPA or waiver request. Nebraska launched in May 2026 with Montana and Iowa implementing in July and December 2026, respectively.
Individuals who submit a new application on or after January 1, 2027 (or an earlier start date at state option) will be required to meet WRRs. Any pending application received on or before December 31, 2026, must be processed according to pre-H.R. 1 eligibility rules.
For current enrollees, states must require applicable individuals to demonstrate compliance with WRR at the enrollee’s first renewal “initiated” on or after January 2027. Generally, states initiate the renewal process 60 to 90 days prior to the renewal month. This is when they gather and review data to verify eligibility, to the extent possible, before requesting information from the enrollee. The IFR clarifies that states may start assessing WRR compliance for renewals “initiated” in January 2027. In all states, except the few that implemented WRRs early, the first batch of renewals subject to WRRs will be for enrollees with March or April renewal dates that are initiated in January.
The rule aligns with guidance allowing states to begin conducting semi-annual renewals (as required by H.R. 1 for expansion enrollees) with renewals initiated in January 2027, which would stagger renewals over a 12-month period. For semi-annual reviews, states also have the option to reschedule renewals for individuals enrolled in January as close to a 6-month renewal cadence as possible. Expediting renewals at the same time WRRs are implemented would add to the already untenable administrative burden on states. A more logical approach would be to use current renewal dates and stagger implementation of both semi-annual renewals and WRRs over the course of a full year.
State Outreach Requirements
States must target outreach directly to expansion adults (§ 435.561(a)). States should only conduct WRR outreach to individuals enrolled or eligible to enroll as an expansion adult (adults in Medicaid expansion coverage or applicable Section 1115(a)(2) waiver program) who are between 19 and 64 years old, who are not pregnant, and who are not dually eligible for Medicaid and Medicare.
Initial outreach notices must be sent three months prior to a state’s implementation date plus the length of a lookback period at application (§ 435.561(b)) (e.g., 4 months prior to implementation in states with 1-month lookback). Between initial outreach notice and the state’s WWR implementation date, states must conduct periodic outreach whenever the state acts on eligibility information.
Periodic notices are also required in several instances (§ 435.561(b)(3)):
- After a redetermination at application or renewal, or a change of circumstance;
- When the state adopts or drops a short-term hardship exception (§ 435.561(b)(3)(ii) – (iv));
- When an emergency/disaster declaration occurs or a high unemployment short term hardship is available (notice to affected enrollees indicating the short term exception becomes available to local residents);
- When an individual is determined to no longer be a Specified Excluded Individual;
- If requested by CMS, when state monitoring data reflects a need for increased outreach.
Outreach notices must be provided in a manner consistent with standing rules at § 435.905(b) on accessibility of program information (§ 435.561(c)). Notices must be sent by mail or electronically (if opted by the individual) and in one other modality, including the individual’s online account, telephone, text message, or other commonly available electronic means. A generic notice on the state’s website does not satisfy this requirement. The notice must explain:
- How to comply with WRRs;
- If the state has adopted short-term hardship exceptions;
- Who is an applicable individual and who may be excluded or excepted;
- The number of months the individual must demonstrate compliance;
- How the state will verify compliance;
- The consequences of non-compliance, including loss of eligibility for premium tax credits in the Health Insurance Marketplace;
- How to report a change that may affect the individual’s status.
Managed Care Implications (§§ 438.58; 435.561(e)(2))
CMS encourages states to leverage Medicaid managed care organizations (MCOs) to support outreach and educate members about WRRs, and to share data that helps the state verify exclusions or exceptions for medical reasons. CMS notes that data sharing is critical for ensuring the state has up-to-date information about an enrollee’s medical frailty status or participation in a drug or alcohol treatment program. States may also use managed care plans to periodically provide outreach notices that inform members of WRRs through various modalities (e.g., regular mail, text, or email) (§ 438.561(e)(2)). If a state chooses to do this, it must instruct MCOs on who should receive the notices, how frequently they should be sent, and their exact content. These types of administrative tasks may be included in the MCO’s capitation rates.
Consistent with current law, states may not delegate key eligibility duties to MCOs, such as determining an enrollee’s compliance with WRRs or issuing noncompliance notices (§ 438.58). MCOs may perform other activities—such as providing referrals to work programs—but the costs of these activities may not be included in the calculation of capitation rates. However, if work referral activities meet the Medicaid definition of value-added services, related costs could be included in the medical loss ratio numerator as incurred claims.
Data and Monitoring
States must report data that is timely, complete, and of sufficient quality, as specified by CMS, for the purpose of monitoring implementation and administration of WRRs (§ 435.562(c)). The IFR sets out five specific categories of data states must report, but for the most part, the required data elements in the IFR are already required in the Medicaid performance indicators that states already report to CMS (see Table 2). The IFR does not specify that these data be disaggregated for the expansion adults, which limits their usefulness considerably. Performance indicators are published by CMS monthly with a 3-month lag. Posting of enrollment data for expansion adults is generally released with a 6-month lag, which makes them less useful for timely monitoring and rapid response.
After publication of the IFR, CMS updated the Medicaid and Children’s Health Insurance Program Eligibility Processing Data report, which includes more details on the data that states must report for monitoring WRR implementation. See Table 3 below.
While the updated data in the Medicaid/CHIP Eligibility Processing Data report will provide some insight into what happens to expansion adults at renewal, more data is needed. Ideally, CMS should:
- Require states to disaggregate the performance indicator data by major Medicaid groups: 1931 parent/caretaker relatives, expansion adult, child, and pregnant or postpartum.
- Require more detail on the reasons for denials or disenrollment to help identify issues and areas in need of improvement.
- Require states to report the number of expansion adults up for renewal. The data listed above are incomplete without a denominator – the total number of expansion adults up for renewal. While the different outcomes (compliance, deemed compliant, disenrolled, etc.) could be added to estimate the renewals due, there is no way to confirm that the numbers are correct without an applicable denominator. To make the data most relevant and useful, WRR data reporting should start with a total count of the number of expansion adults up for renewal.
- Require states to disaggregate the number of expansion adults who demonstrated compliance or were deemed compliant based on ex parte data or via submission of information. These data are reported for the total Medicaid MAGI population and should be reported separately for those impacted by WRRs to assess a state’s relative success in verifying compliance with data available.
- Require further disaggregation of data, particularly regarding medical frailty, to identify barriers to enrollment and retention for these vulnerable individuals. For example, if the ex parte rate is substantially lower than that for all expansion adults, the data can be analyzed further to identify process and data improvements.
- Require states to disaggregate the number of expansion adults who requested fair hearing requests for disenrollment, including fair hearing requests pending for more than 90 days.
Conclusion
The implementation of WRRs will pose incredible burdens on state Medicaid agencies and take away health care from millions of very low-income and vulnerable individuals. States may also spend large sums of taxpayer dollars on for-profit consultants and vendors to implement these complex rules as was the case in the state of Georgia’s rollout of work reporting requirements. Policymakers passed a law that undermines the purpose of Medicaid and punishes states that have expanded Medicaid to low-income adults and parents who do not have access to affordable coverage. Moreover, the complexity of the rules means it will be near impossible for the millions of low-income Americans who rely on Medicaid for their access to health care to understand them. Providers who serve Medicaid populations will face new burdens further threatening provider participation rates.
When the law was being debated, lawmakers knew the consequences would be severe: the Congressional Budget Office estimated that 5.3 million adults would lose Medicaid coverage due to WRRs. But the Trump Administration has made it worse by adding extra stringent and onerous mandates for medically frail individuals, those who need health care the most.
The unexpected changes in the IFR turns what was already an unreasonable timeline into the impossible; without additional time to prepare, states will likely default to paperwork and manual processing creating more administrative burden, which relies on timely and reliable delivery of mail from the U.S. Postal Service that has been plagued with problems particularly in rural areas. Manual processing is also prone to human errors and lost paperwork, not only for the state, but also for individuals, health care providers, and health plans. The threat of audits to determine whether or not state definitions and verification processes fully complied with the regulations without clear federal rules in place will result in states potentially over-verifying to avoid the high-stakes risk of eligibility errors. Ultimately, the fallout will not be limited to expansion adults. When states get backlogged with red tape and burdensome paperwork, all Medicaid enrollees or new applicants will be at risk of losing health coverage, even children, seniors, and people with disabilities who were allegedly protected.
Appendix A: Using MAGI Income Counting Rules
For the purposes of determining income for WRR compliance, states must use the same MAGI standards used for financial eligibility of Medicaid (§ 435.552(f)). The IFR directs states to use MAGI income, which includes only taxable income sources plus a few adjustments. For tax filers, MAGI starts with the adjusted gross income (AGI) on a federal tax return. Non-taxable Social Security benefits for adults, tax exempt interest, and excluded foreign income, are added to the AGI to determine the household MAGI income. The household size is the size of the tax filing unit. For non-tax filers, income is calculated in the same way, but the household size is based on immediate family members living together.
Using MAGI for WRRs builds on how states determine income for eligibility purposes, but MAGI doesn’t treat everyone equally. Here are a couple of examples:
Example 1: Taxable v. non-taxable income sources. MAGI excludes non-taxable income sources such as supplemental Social Security Income (SSI), TANF and other cash assistance, tax refunds or refundable tax credits, worker’s compensation payments, veteran’s benefits, child support, gifts and loans, and proceeds from life insurance or inheritances.
An unemployed adult receives $600 a month in unemployment compensation, which is taxable and counts as MAGI income for WRR compliance and financial eligibility.
A partially disabled veteran receives $600 a month in veteran’s benefits or a construction worker receives $1,000 in worker’s compensation. Neither of these sources of income counted toward MAGI. These individuals would have to show compliance through other work or qualifying activities. The injured worker might be Specified Excluded as medically frail but because the veteran is only partially disabled and his VA benefits are not counted, this individual will need to meet WRRs in other ways.
Example 2: Child support is not counted as MAGI income for financial eligibility or WRR purposes. In some cases, this helps lower income parents qualify for 1931 coverage by excluding child support. However, in 15 states with the lowest 1931 eligibility levels, a swath of parents have income above 1931 eligibility levels but below the $580 income proxy for work compliance. These parents will need to have other qualifying activities to meet WWRs even though child support would put the household income above $580.
A single parent with two children earns $300 per month and receives $1,200 per month in child support. The state’s upper income eligibility for 1931 parents is 12% FPL or $273 per month for a family of three, therefore this parent is considered an expansion adult and subject to WRRs. If child support were counted, this parent would be in compliance using the $580 proxy rule. But since it is not counted as MAGI income, the parent will have to demonstrate compliance another way unless they qualify for an exception or exclusion.
A single parent with two children earns $2,500 per month and receives $800 in child support. If child support isn’t counted, the household MAGI income is $2,500 and the parent is eligible for expansion and meets WRRs through the income proxy. But if child support were counted, the income would be $3,300 and over the monthly income limit of $3,142. This parent would no longer be eligible for Medicaid expansion coverage.
Appendix B: Considerations for Presumptive Eligibility
Hospitals and other qualified entities that are authorized to make presumptive eligibility determinations must screen for compliance of WRRs as an eligibility factor in their determinations. Presumptive Eligibility (PE), if adopted by the state, allows designated qualified entities, such as health clinics, to temporarily enroll individuals in Medicaid based on a preliminary review of all eligibility criteria, including income. Hospital Presumptive Eligibility (HPE), which is at a hospital’s discretion, enables hospitals to make preliminary assessments of Medicaid eligibility. Under the IFR, qualified entities now have added duties to screen for compliance with WRRs – or exclusion or exception from WRRs – as part of PE and HPE determinations.
PE and HPE determinations continue to be based on attested information from the applicant. CMS requires qualified entities to “assess and obtain an attestation” as to whether the individual appears to be a Specified Excluded individual, an applicable individual, or meets a mandatory or short-term hardship exception. If the individual is an applicable individual, the qualified entity must evaluate whether the individual complied with WRR in the month prior to month of application (or up to three prior months if the state elected a longer application lookback period). CMS notes that the applicant “must attest” to such compliance.
States will have to update their PE and HPE training materials, update PE and HPE application materials and eligibility determination notices, and train PE and HPE qualified entities on the new requirements.
Endnotes
- CMS clarifies that individuals in other waiver demonstrations, such as Section 1915(b), 1915(c), or 1115(a)(1) waivers, are not applicable individuals and not subject to WRRs. 91 Fed. Reg. p. 33353. WRRs also do not apply to demonstrations that provide limited Medicaid benefits, such as family planning-only benefits to individuals eligible under Section 1115(a)(2) family planning demonstrations. ↩︎
- In the preamble, CMS notes “there will be circumstances in which no documentation exists, or documentation is not reasonably available. For example, an individual who lives with and provides regular assistance to their disabled parents may qualify for an exclusion on the basis of being a family caregiver. Because of the personal nature of this type of assistance, it often occurs outside of an employer/employee or other contractual relationship. As such, an individual is unlikely to have documentation to provide that demonstrates qualification for the exclusion….”(91 Fed. Reg. 33395). ↩︎
- ICD-10 is a common standardized system used by health care providers to code and classify diseases and medical conditions. ↩︎
- For an NEA emergency, while the IFR does not explicitly require CMS approval, the rule notes that “CMS will review states’ use of and implementation of [this] exception” (§ 435.555 (d)(2)(iii)). For Robert Stafford Act disasters, even though a disaster declaration does not expire for purposes of federal funding authorization, the “incident period” is a designated number of days or3- weeks specified by FEMA. States must apply the disaster hardship to all residents living within the designated disaster area for the month or months during which the identified incident period occurred. While initial CMS approval is not needed, states may request CMS approval to extend the exception beyond the incident period by providing documentation that barriers to meeting work reporting requirements in the relevant area persist (e.g., structural damage, relocations, business closures or destroyed transit infrastructure) (§ 435.555 (d)(2)(iv)). ↩︎
- Retroactive coverage is federal policy allowing Medicaid to pay medical bills for one or more months before an individual’s application date. Retroactive coverage is especially helpful in emergencies or during sudden health crises where individuals cannot apply for coverage immediately. H. R. 1 reduced the maximum retroactive eligibility period for applicants from three months prior to the application month to one month for Medicaid expansion adults and two months for other Medicaid groups. To qualify, you must have been eligible for Medicaid during that period and received services covered by the program. Thus, even with retroactive coverage, an individual who experienced a hospitalization in March and applied for Medicaid in April must still show they were eligible for Medicaid in March – including that they complied with WRR in thelookback month of February. ↩︎
- For WRR purposes, the two income counting methods can result in different outcomes. For example, Max is employed from April through September earning $1,500 per month. States counting reasonably predictable changes in income smooths out income fluctuations. Regardless of when the individual applies, the prorated monthly income is $750 per month (6 x $1500 / 12) which is more than the $580 proxy and complies with WRRs. In contrast, using six month averaging can produce different results based on time of application or renewal: Max applies for Medicaid in August. The preceding six months would be February – July, during which Max worked 4 months, earning a total of $6000 / 6 months = $1,000 monthly income and he qualifies. But when Max renews coverage in February, the 6-month lookback is August – January when Max only worked two months, he would no longer qualify just for work because his average income is below $580 ($3,000 / 6 = $500). ↩︎
- While claims data typically includes a provider’s bill or amount for payment, encounter data documents the delivery of medical care or services and diagnoses, but may not necessarily include a payment amount because the provider is already being paid through a capitated or pre-negotiated budget. ↩︎
- If an individual is denied or disenrolled specifically for not complying with WRRs as opposed to other eligibility criteria, they will not be eligible to receive premium tax credits to purchase a Health Insurance Marketplace plan. The law and rule did not indicate how long this prohibition lasts or how the state must inform the marketplace of the exclusion. In the rule, CMS indicated that information would be released on this provision in further guidance. ↩︎